BRIEF REPORTS
HEAD INJURY REHABILITATION OUTCOME IN RELATION TO THE CARERS’ PSYCHOLOGICAL DISTRESS
Rukhsana Kausar*, Chris Fife-Schaw**, Sara Hampson***, Martin Van den Broek****
ABSTRACT
Carers are the backbone in providing care in the community and in doing so, it takes a heavy emotional toll. Therefore, the psychological health of the carer is important for community rehabilitation of people with head injury. The present study was conducted to examine post head injury rehabilitation outcome in relation to psychological distress in the carers. It was hypothesised that carers’ psychological distress would predict the functioning of affected people. People with head injury were recruited from the rehabilitation unit as well as outpatient clinics in Atkinson Morley Hospital, London. Brain Injury Community Rehabilitation Outcome (BICRO-36) was used for assessment of the physical, emotional, cognitive and social functioning, which was carried out by the carers. Psychological distress in carers was assessed using General Health Questionnaire (GHQ-28). Data was analysed using t-test, one way analysis of variance, correlation and regression analyses. Psychological distress in carers was significantly associated with rehabilitation outcome of people with head injury. The findings have important implications for policy makers, health care professionals, for people with head injuries as well as their families.
INTRODUCTION
Severe head injuries are the commonest cause of death in young men in UK and the USA (1). Head Injury (HI) can lead to numerous difficulties in areas that include activities of daily living, cognitive functioning, emotional and physical functioning. The longstanding residual effects of Traumatic Brain Injury (TBI) include cognitive, social and personality changes (2,3,4,5,6). Such implications of head injury not only have a significant impact upon the lives of survivors but also upon the lives of their family members and carers (7, 8)
Those discharged from hospitals and rehabilitation units following a TBI return to live mainly with their families (9). The informal care network of family and friends has become one of the most important elements in supporting individuals with brain injury, in their local community. Usually, it is one person (typically the wife or mother) who takes on the major responsibility of care.
Family members experience a high level of distress, guilt and burden (7, 10, 11) . Stress experienced by the carers may interfere with their ability to assist with the affected person’s rehabilitation activities. It has been realised for more than a decade that families providing care to a person with head injury should be considered as an integral part of the rehabilitation team, as they are a source of motivation and adaptation for the person (12, 13). Moreover, family involvement, cooperation, and particularly their commitment to follow through with the rehabilitation process in the home setting are absolutely necessary to the long-term rehabilitation of head injury and the family system. There is a need to emphasise upon the carers’ psychological functioning. Such studies would provide knowledge and assistance to those professionals involved in rehabilitation.
The main objectives of the present study were to assess: psychological distress in carers of head injured persons; to assess head injury outcome in terms of physical, psychosocial, emotional and cognitive functioning of the affected person and to examine relationship of carers’ psychological functioning with head injury outcomes. It was hypothesised that: a.) the carers of head injured persons experience psychological problems such as anxiety, depression, somatic problems and social dysfunctioning; b. carer distress predicts rehabilitation outcome of head injured persons.
METHOD
Participants and Recruitment
The sample comprised 42 carers of a community dwelling former clients of a neurosurgery, neurology and rehabilitation centre. The clients were recruited through St George’s Healthcare NHS Trust. Carers of these people who ranged in age from 18-65 years, lived in a non- institutional community setting and had acquired head injury 4-18 months prior to the assessment were included.
Head injuries in the majority had resulted from motor vehicle accidents (54.8%) and from falls (33.3%). A majority of the patients were male (76%) with the mean age of 38 years (SD = 12.37) and were single (40.5%). Most of them had been employed full time preonset (72.5%), whereas after head injury 25% were working full time and about 30% were unfit for work. Severity of injury varied from mild to severe and most of them had experienced mild head injury (54.8%). Carers mainly comprised of females (73.8%) and half of them were parents.
Measures
Psychological distress in carers was measured using General Health Questionnaire (GHQ- 28) (14). Severity of head injury was estimated through Glasgow Coma Scale score as provided in the hospital records. Head injury outcome was assessed in terms of the patient’s physical, psychosocial, emotional and cognitive functioning (memory) using the Brain Injury Community Rehabilitation Outcome (BICRO-36) scales. BICRO includes eight subscales: Personal Care, Mobility, Self-organisation, Partner and family contact, Parents and children contact, Socialising, Productive employment and Psychological Well-being. A relatives’ questionnaire (15) was used to assess memory deficits and emotional problems in the affected person. High scores on all BICRO scales indicated either deficits or problems in respective areas of functioning, except for Psychological well-being scale where the high score meant better psychological functioning.
Procedure
Two packets, one for the person with head injury and one for the carer, were either mailed or handed over to them at out-patient clinics. The packet for the affected person contained a letter from the researcher explaining the nature and purpose of the study and consent forms. The person was requested to sign the consent form and pass on the carers’ envelope to them if they themselves were willing for carers to participate. Carers were requested to complete and send questionnaires back to the researcher in Freepost envelopes provided to them. The response rate was 24.58%.
RESULTS
Psychological Distress in Carers
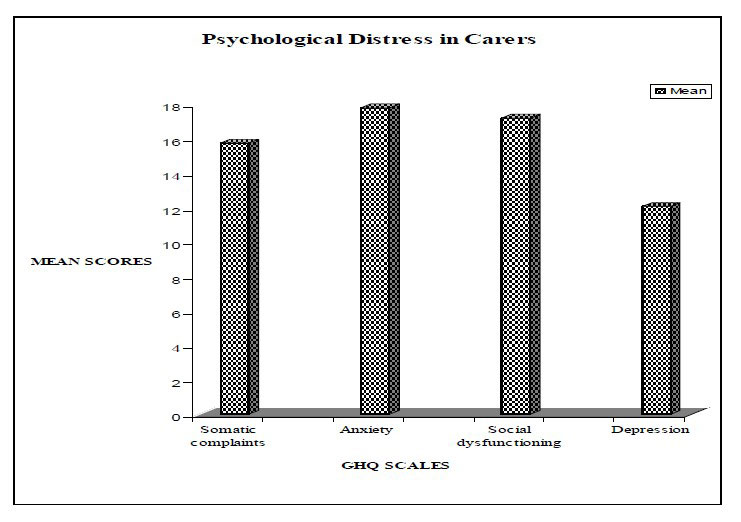
Mean scores on four subscales of GHQ showed that carers experienced anxiety followed by social dysfunctioning and somatic complaints (Figure.1).
Pearson Correlation analysis was used to examine relationship of head injury, and carer affected person variables, with carers’ distress. Severity of head injury had positive correlation with somatic complaints (g = .58, p<0.001), anxiety (g = .36, p<0.05) and social dysfunctioning (g = .36, p<0.05) in carers. Duration of carers’ acquaintance with the person prior to the onset of head injury had negative relationship with depression in carers (g = - .31, p< 0.05).
One-way analysis of variance was carried out to examine whether distress in carers differed as a function of carers’ relation with the patient. The carers’ relation with the patient had a significant effect on depression in carers (F = 5.94, df = 2(39), p<0.001). Post-hoc analysis revealed that parent carers were significantly less depressed than spouse and partner carers (t = 3.34, df = 40, p<0.002, M1 = 9.47, SD1 = 2.74, M2 = 14.66, SD = 6.55 for both groups respectively). Partner and spouse carers did not differ in the psychological distress they experienced.
Figure 1. Psychological distress in carers (N = 42)
{kind=link}
Rehabilitation Outcome in Affected Persons
Multivariate analysis of variance with repeated measures revealed significant differences in physical, psychological, social, emotional, cognitive and employment outcome (F = 50.48, p<0.001). Emotional problems were reported as major ones followed by socialisation problems, psychological well being, productive employment, self-organisation and memory deficits. However, very few problems were reported in the areas of cognitive functioning, personal care, mobility and relations with family members.
Severity of head injury showed no relationship with any of the patient outcome variables, except for ability of personal care ( =.34, p< 0.05). Duration of carers’ acquaintance with the person before the onset of head injury had negative correlation with the person’s relationship with parents and siblings (g =-.40, p<0.01). Time since onset of head injury had negative relationship with ability of personal care (g =-.34, p<0.05) in affected persons.
Carers’ distress and rehabilitation outcome in affected persons
Table I presents correlations between measures of rehabilitation outcome and carers’ psychological distress. High scores on outcome variables indicate more problems in a particular area. Somatic complaints in carers had positive correlation with problems in areas of self organisation, parent family relations, productive employment and emotional problems. Carer anxiety was significantly correlated with emotional problems and memory deficits in the affected persons. Social dysfunctiong in had strong association with problems in selforganisation, parent-family relations, socialisation and productive employment. Carer depression had significant correlation with self-organisation, socialisation and productive employment. Psychological well being of affected persons had significant negative correlation with all carer distress variables.
| Somatic Complaints | Anxiety Social-dysfunction | Depression | |||
|---|---|---|---|---|---|
| 1. | Personal care | 0.18 | 0.11 | 0.18 | 0.02 |
| 2. | Mobility | 0.02 | 0.08 | 0.22 | 0.22 |
| 3. | Self-Organisation | 0.49*** | 0.22 | 0.71*** | 0.58** |
| 4. | Parent and family relations | 0.31* | 0.10 | 0.33* | 0.10 |
| 5. | Parent and sibling relations | 0.11 | 0.05 | 0.13 | 0.29 |
| 6. | Socialization | 0.24 | 0.24 | 0.32* | 0.52*** |
| 7. | Productive employment | 0.34* | 0.06 | 0.55*** | 0.31* |
| 8. | Psychological well being | -0.51** | -0.46** | -0.45** | -0.33* |
| 9. | Cognitive problems | 0.11 | 0.23 | 0.00 | 0.17 |
| 10. | Emotional problems | 0.38* | 0.40** | 0.12 | 0.29 |
| 11. | Memory deficits | 0.30 | 0.38* | 0.04 | 0.30 |
*p<0.05, **p<0.01, ***p<0.001
Further to correlation analyses, regression analysis was carried out to examine predictors of rehabilitation outcome. Severity of injury and carer distress variables were entered as predictors in a separate set of analysis for each outcome variable using hierarchical regression. Table 2 shows the steps in which the variables were entered, the standardised regression coefficients (betas) and the proportion of variance explained at each step. In all equations, severity of head injury explained very little variance, whereas addition of carer distress variables significantly added in variance explained for outcome variables i.e. selforganisation, parent family relations, socialisation and productive employment.
| Step | Out come variable | Predictor Variable(s) | ?R2 | Beta |
|---|---|---|---|---|
| 1. | Personal Care | Severity of injury | .34* | .33 |
| Somatic complaints | .32 | |||
| Anxiety | .01 | |||
| Social dysfunctioning | .41* | |||
| Depression | .06 | |||
| R2 | .11 | .25 | ||
| R2 change | .13 | |||
| F change | 1.41 | |||
| 2. | Self-oganisation | Severity of injury | .24 | .03 |
| Somatic complaints | .11 | |||
| Anxiety | .27 | |||
| Social dysfunctioning | .56** | |||
| Depression | .35* | |||
| R2 | .06 | .60 | ||
| R2 change | .54*** | |||
| F change | 10.80** | |||
| 3. | Parent family relations | Severity of injury | .04 | .38* |
| Somatic complaints | .72** | |||
| Anxiety | .25 | |||
| Social dysfunctioning | .26 | |||
| Depression | .30 | |||
| R2 | .002 | .25 | ||
| R2 change | .25* | |||
| F change | 2.70* | |||
| 4. | Parent sibling relations | Severity of injury | .17 | .42** |
| Somatic complaints | .78** | |||
| Anxiety | .16 | |||
| Social dysfunctioning | .25 | |||
| Depression | .79*** | |||
| R2 | .03 | .41 | ||
| R2 change | .38** | |||
| F change | 5.17** | |||
| 5. | Socialisation | Severity of injury | .13 | .12 |
| Somatic complaints | .48* | |||
| Anxiety | .67** | |||
| Social dysfunctioning | .15 | |||
| Depression | .69** | |||
| R2 | .01 | .33 | ||
| R2 change | .31** | |||
| F change | 3.82** | |||
| 6. | Productive employment | Severity of injury | .22 | .02 |
| Somatic complaints | .31 | |||
| Anxiety | .34 | |||
| Social dysfunctioning | .52** | |||
| Depression | .01 | |||
| R2 | .05 | .40 | ||
| R2 change | .35** | |||
| F change | 4.71 |
*p<0.05, **p<0.01, ***p<0.001; Mobility, psychological well-being, memory, cognitive and emotional problems in patients were not predicted by any of the antecedents.
Severity of head injury predicted affected persons’ ability of personal care when entered as a single predictor in the first step and the person’s interpersonal relationship with the family only when entered in combination with carer distress variables in the second step of equation. Carer distress variables differentially predicted affected persons’ functioning. Carer social dysfunctioning predicted ability of personal care, self-organisation and productive employment. Carer depression predicted affected persons’ self organisation ability as well as their social and interpersonal relations.
Somatic complaints in carers emerged as significant predictor of affected persons’ social and interpersonal relationships. Carer anxiety predicted the person’s ability to socialise. None of the carer distress variables predicted mobility, psychological well-being, emotional problems, cognitive deficits and memory deficits in affected persons.
DISCUSSION
The present study examined rehabilitation outcome of head injury in relation to psychological distress in carers. Similar to other head injury family studies the primary caregivers in this study were predominately female and parents (7,11, 16).
Carers experienced psychological distress in the form of somatic complaints, social dysfunctioning and anxiety. Findings pertaining to distress reported in carers, are in line with existing literature which has extensively investigated psychological outcome of head injury care (17-18). Severity of injury showed positive correlation with carer depression. This finding substantiates earlier research (19) which revealed that more severe injuries were related to greater psychological distress and anxiety in relatives. Carers who had known the affected persons for a longer period were less depressed. Moreover, parent carers reported less depression compared to spouse and partner carers. Many researches have suggested that caregiving spouses in TBI population are at greater risk for distress, than caregiving parents (2, 17, 20, 21, 22). One possible explanation for the parent carers reporting less depression could be that parents had already been involved in caregiving to the person as their child, whereas for spouse and partner carers, assuming a new and different caregiving role is more difficult. The parents are likely to have more support and be less financially threatened (21). For spouses and partners, personality and emotional changes in affected persons would make it more difficult to cope with. Their needs for sexual and affectional desires, intimacy and empathy in communication with spouses may be unmet, yet they would feel guilty about getting separated or divorced in such circumstances (23).
Carer distress showed positive correlation with rehabilitation outcome. Affected persons’ ability of self-organisation, interpersonal problems, productive employment and psychological well-being seemed to be a major concern for carers as distress in carers showed significant correlation with deficits in these areas. Ability of self-organisation, interpersonal relationships and psychological well being are important factors for productive employment. Majority of the affected persons in this study were young adults who had been working fulltime (69%) prior to the injury. However, after the injury their work status had either been changed or they had become unemployed and only 10 % could come back to their full-time work status. Carer anxiety had significant association with psychological problems in affected persons such as psychological well-being, emotional problems and memory deficits. These findings are consistent with the TBI literature which has emphasised that impact of psychosocial, emotional and cognitive sequelae on carers is more than physical complaints (11, 15).
Regression analysis revealed that except for ability of personal care, the severity of injury did not predict outcome. However, psychological distress in carers predicted affected persons’ current functioning. Carer distress predicted the ability of self-organisation, productive employment and interpersonal relationships in affected persons. All these abilities are important for reinstating the work-status of affected person. Having considered that majority with HI in this study were young adults who were at the peak of their professional and practical life, this finding holds utmost importance from a rehabilitation point of view. There is extensive research which has looked at correlates of psychological distress in carers (24, 25), however, psychological distress as an antecedent of rehabilitation outcome has not been investigated. The findings of the present research emphasise the importance of carer psychological well being in rehabilitation of persons with TBI in the community.
One major limitation of the present study is that assessment of affected persons’ current functioning was carried out by the carers and there was no objective measure used for this purpose. Carer assessment could be their subjective perception and not related to the actual deficits in the affected persons (26). Secondly, though an effort is made to establish that carer psychological distress is a predictor of functioning in the affected person, cross-sectional research has an inherent limitation in establishing cause and effect relationship. Future research needs to adopt a longitudinal design and use objective assessment methods for studying psychological and physical functioning of persons with head injury.
* Address for correspondence:
Department of Psychology and Applied Psychology
University of the Punjab
Lahore, Pakistan
Phone No +0092- 42-9231245
Email: rukhsana.saddul@gmail.com
** Psychology Department, School of Human Sciences
University of Surrey, U.K.
*** Psychology Department, School of Human Sciences
University of Surrey, U.K.
****Wolfson Neurorehabilitation Centre
Atkinson Morley Hospital, St. George’s NHS Hospital, London, U.K.
ACKNOWLEDGEMENT
This research was part of a post-doctoral project carried out at the Surrey University and the Wolfson Neurorehabilitation Centre, St. Georges’ NHS Trust (London). This project was financially supported by the Association of Commonwealth Universities.
REFERENCES
- Fraunlic A, Horta E, Maturana R, Scherpenisse J, Carbonell C. Organic personality Disorder after traumatic brain injury: cognitive, anatomic and psychosocial factors. A 6 month followup. Brain Injury, 14 (5), (2000), 431-439.
- Maus-Clum N, Ryan M. Brian injury and the family. Journal of Neurosurgical Nursing, 13 (1981), 165-169.
- Dikmen S, Reitan R, Temkin N. R. Neuropsychological recovery in head injury. Archives of Neurology, 40 (1983), 333-338.
- Fletcher J M, Ewing-Cobbs L, Miner E M, Levin H. S, Eisenberg H M Behavioral Changes after closed head injury in children. Journal of Consulting and Clinical Psychology, 58 (1990), 93-98.
- Levin. Neurobehavioral recovery. Journal of Neurotrauma, 9 (Suppl. 1) (1992), S359-S373.
- Kausar R Head Injury and its Psychological Implications: a literature review. Pakistan Journal of Neurology, 2 (1996), 17-20.
- Brooks D N The head-injured family. Journal of Clinical and Experimental Neuropsychology, 13 (1991), 155-188.
- Perlesz A, Kinsella G, Crowe S. Impact of traumatic brain injury on the family: A critical review. Rehabilitation Psychology, 44 (1) (1999), 6-35.
- Jacobs H E The Los Angeles and head injury survey: procedures and preliminary findings. Archives of Physical Medicine and Rehabilitation, 69 (1988), 425-431.
- Medical Disability Society: Working party report. The management of traumatic brain injury (London: the development trust for the young disabled on behalf of the Medical Disability Society) (1988).
- Kausar R, Powell G E. Subjective Burden on Carers of Patients with Neurological Problems as a Consequence of Objective Symptoms (Objective Burden). Clinical Rehabilitation, 10 (1996), 75-81.
- Brown B W, McCormick T. Family coping following traumatic head injury: an exploratory analysis with recommendations for treatment. Family Interventions, 37 (1988), 2-16.
- Kinsella G, Ong B, Murtagh D, Prior M, Sawyer M. The role of family for behavioural outcome in children and adolescents following traumatic brain injury. Journal of Consulting and Clinical Psychology, 67 (1), (1999), 116-123.
- Goldberg D. P, Williams P. User’s guide to the General Health Questionnaire. Windsor, Berkshire, England: Nefer-Nelson. (1988).
- McKinlay W W, Brooks D N, Bond M R, et al. The short term outcome of severe blunt head injury as reported by relatives of the injured person. Journal of Neurology, Neurosurgery and Psychiatry, 44 (1981), 527-533.
- Florian V, Katz S. The other victims of traumatic brain injury: Consequences for family members. Neuropsychology, 5(4) (1991), 67-279.
- Kreutzer J S, Gervasio A H, Complair P S. Primary caregivers’ psychological status and family functioning after traumatic brain injury. Brain Injury, 8(3) (1994), 197-210.
- Moulse S, Chandler B J. A study of the health and social needs of carers of Traumatically brain injured individuals served by one community rehabilitation team. Brain Injury, 13(12), (1999), 983-993.
- Livingston M G, Brooks D N, Bond M R. Three months after severe head injury: Psychiatric and social impact on relatives. Journal of Neurology, Neurosurgery and Psychiatry, 48 (1985), 870-875.
- Gervasio A H, Kreutzer J S. Kinship and family members’ psychological distress after traumatic brain injury: A large sample study. Journal of Head Trauma Rehabilitation, 12(3), (1997), 14-26.
- Hall K M, Karzmark P, Stevens M, Englander K, O’Hare P, Wright J. Family stressors in traumatic brain injury: A two years follow up. Archives of Physical Medicine and Rehabilitation, 75 (1994), 876-884.
- Leatham J, Heath E, Woolley C. Relatives’ perceptions of role change, social support and stress after traumatic brain injury. Brain Injury, 10(1) (1996), 27-38.
- Doka K J. Disenfranchised grief: Recognizing hidden sorrow. Lixington M.A. Lexington Brooks, (1988).
- Perrot S B, Taylor H G, Motes J L. Neuropsychological sequelae, familial stress, and environmental adaptation following pediatric head injury. Developmental Neuropsychology, 7 (1991), 69-86.
- Gray J M, Shepherd M, Mckinlay W W, Robertson I, Pentland B. Negative symptoms in the traumatically brain injured during the first year postdischarge, and their affect on rehabilitation status, work status and family burden. Clinical Rehabilitation, 8 (1994), 188-197.
- Nolan G, Grant G, Ellis N. Stress is in the eye of the beholder: reconceptualising the measurement of carer burden. Journal of Advanced Nursing, 15 (1990), 544-555.