PERCEPTION OF PHYSIOTHERAPY AND OCCUPATIONAL THERAPY STUDENTS SUPERVISION OF FIELD ATTACHMENT IN ZIMBABWE
Vyvienne RP M’kumbuzi*, Tamisayi PT Chinhengo, Farayi Kaseke
ABSTRACT
The field attachment for physiotherapy (PT) and occupational therapy (OT) students at the University of Zimbabwe has evolved since its inception in 1987. The new design places demands on local supervisors to ensure that all objectives are covered well. The purpose of this study was therefore, to evaluate PT and OT students’ experiences of the quality of supervision of a rationalised field attachment programme.
A 4 - year (2004 ? 2007) longitudinal survey was conducted by a direct questionnaire. Modal scores for the quality of local supervision were calculated for each broad objective of the attachment. The supervisors’ mark was regressed against the field attachment average obtained by the student, as an indicator of the level of critical analysis of the student’s performance by the supervisor.
One hundred and eight PT and OT students participated in the study. The modal total quality rating over the four years was 62.5% (IQR = 53.1% - 68.8%). Factors associated with a high total quality rating for supervision were constant supervision (p<0.01), the year 2005 (p<0.01. Occupational therapy students tended to rate their supervisors higher (p=0.03). Local supervisors tended to overrate student performance contributing 49% variance to the field attachment average mark (p<0.01).
Although students experienced good quality supervision, training of local supervisors in methods and frequency of supervision and in evaluating students were suggested to improve supervision. A review of the weighting of the field attachment evaluation components was recommended.
INTRODUCTION
Fieldwork prepares students to work in emerging practice areas and meet standards of accreditation. It also enables teachers to examine the current field work systems and give recommendations (1).
The field attachment programme is an important feature of all degree programmes (PT, OT, MBChB, Pharmacy, Nursing Science and Dentistry) in the College of Health Sciences at the University of Zimbabwe. It places significant emphasis on a social approach to health care which is increasingly acknowledged as a credible approach to decreasing morbidity and mortality(2), and is also being encouraged by the Ministry of Health and Child Welfare in Zimbabwe. The cost of health care, the burden of disease in a mixed epidemiological transition and the high burden attributable to HIV/AIDS has necessitated an increase in the quality of community care approaches(3). Health science students need to be exposed to best practice during community training. This can be ensured through adequate supervision. A Zimbabwean study demonstrated how supervised projects in a community based clinical pharmacy teaching, research and service programme enhanced pharmacy services, which in turn enabled the development of new clinical attachment sites for pharmacy students (4). Student feedback is said to be helpful and informative towards development of programmes and activities of medical education. It allows students to highlight the weaknesses and strengths of programmes resulting in provision of quality training and education (5).
There is a paucity of published literature on field attachment supervision. However, important inferences can be made from clinical and research supervision. In order for students to achieve a positive learning experience, it is vital that they receive adequate supervision and mentoring. The usefulness of the learning situation depends on several variables such as feedback to students, staff-student relationship, organisation of teaching, meetings with supervisors and supervisors’ characteristics (6, 7, 8). The amount of feedback depends on the way students are supervised, and supportive supervision will redirect the students learning towards areas of efficiency as well as direct subsequent stages.
With regard to research, it was noted that postgraduate students wanted meetings and feedback to be regular and well conducted (8). In South Africa, reporting on undergraduate physiotherapy community based clinical teaching, Taukobong (9) further noted that these students preferred supervisors who are there all the time without necessarily spoon feeding them, as this resulted in increased anxiety in the students. The quality of supervision is perceived by students to be an outcome of the supervisor’s analytical skills. New graduates have been seen to be inexperienced supervisors who may not feel comfortable with community development activities if they have not received adequate training in the area (10). In their study to determine tutors performance rating, Dolmans et al (7) found that tutorial groups’ productivity was an influencing factor in determining tutors performance. Thus groups with low marks rated the tutor low while those with high marks rated the tutor highly. Where the converse was true, it was attributed to some tutors being able to deal with unproductive tutorial groups, whereas others did not possess these skills(11). Tutors with strong group dynamic skills tend to regularly evaluate group function and work to improve cooperation within the group. Tutors’ group dynamic skills contribute positively toward performance scores that they receive from tutorial groups regardless of group performance levels. This is however affected by students’ problem based learning skills, students’ level of prior knowledge and level of functioning in tutorial groups. This finding supports several authors recommendations on the need for training of supervisors in the area of interest and the need for well experienced supervisors who are well informed (6,8,10).
The field attachment programme for Physiotherapy (PT) and Occupational therapy (OT) students at the University of Zimbabwe is aimed at exposing students to the way of life of large scale commercial farming (LSCF), mining, and district, industrial, rural and urban municipal communities.
The field attachment constitutes a seven-week block during the third year of the B.Sc. OT and PT Honours programmes. Students attend formal lectures encompassing Sociology, Psychology, Primary Health Care (PHC), Community Based Rehabilitation CBR) and Administration and Management in preparation for the attachment. Also, by the time the attachment takes place, students have completed their research methodology and biostatistics course and together with their increasing clinical experience are expected to use both quantitative and qualitative analytical approaches to study the communities. Students are also taken through the attachment objectives, and methods of achieving these are suggested and discussed. A pre-prepared handout containing all the relevent information as well as the methods of supervision and evaluation of the field attachment is given to each student prior to their departure.
The combined 3rd year class of PT and OT students is randomly allocated into groups of between three and six students each, and subsequently systematically distributed to provincial and district centres throughout Zimbabwe. The centres are selected on the basis of:1). having experienced rehabilitation personnel who are willing and able to supervise students in situ, and 2). affording accommodation to students.
Rehabilitation personnel in this context include physiotherapists, occupational therapists and rehabilitation technicians (known as PT / OT assistants elsewhere). In addition to this local supervision, an academic member of the staff from the University’s rehabilitation department visits the centres in a supervisory capacity, to give support to the local supervisor and to further their own knowledge of the area. This idea of supervision being necessary because it provides support and upgrades one’s skills has been corroborated, as the supervisor has a threefold role, that of administrator, educator and supporter (10).
The Objectives of the Field Attachment are to:
- Conduct a demographic and socio-economic survey.
- Establish causes and distribution of conditions needing rehabilitation.
- Identify and assess the organisation of health and rehabilitation services.
- Assess characteristics and level of community involvement.
- Describe and participate in Community Based Rehabilitation.
- Participate in and assess the management of a rehabilitation department.
- Describe the roles of staff in the provincial and district health organisation offices.
Students select and engage two or more communities and are expected to conduct a comparative analysis for all the objectives.
The techniques of gathering data are many and triangulation to saturate data is necessary. Data are obtained from many sources including government and specific health officials, traditional, administrative, informal and formal leaders, civic society and lay community members. While a clinical load is not a primary objective, students are encouraged to engage in clinical work and to observe methods of medical and rehabilitation management that are sometimes not a feature of the large academic hospitals where clinical OT and PT teaching occurs. Students therefore need to plan their time well.
Evaluation of the Field Attachment
The marks for the attachment form part of the continuous assessment mark for the course Rehabilitation II. For a student to be deemed eligible to sit for the final examination for this (12). The components of the evaluation include group file, group oral presentation, local supervisor’s assement and peer rating. The detailed criteria and schedule used to evaluate the student is given to the student prior to the field attachment.
Rehabilitation II is a barrier course i.e a student cannot proceed to their 4th year of study if they fail to satisfy examiners in this course (12).
The field attachment programme for PT and OT students in Zimbabwe, in particular the combined placement of PT and OT students, seems to be a unique feature in the training of PT and OT students. There is therefore even less literature to draw from, in this respect. Taukobong et al reported that 65% of physiotherapy students expressed satisfaction with supervision of the community based clinical teaching at MEDUNSA (Medical University of South Africa) (9). Little can be drawn from this study, as the major component was clinical teaching, unlike the field attachment at the University of Zimbabwe. However, the challenges of supervision of community based activities may be similar in some instances, irrespective of the academic content of the activity being supervised.
Statement of the Problem
At inception of the PT and OT programmes in 1987 in Zimbabwe, the field attachment programme extended over 4 years as shown in Table 1.
| YEAR | BLOCK | DURATION |
|---|---|---|
| 1 | Village | 2 Weeks |
| 2 | Rural | 2 weeks |
| 3 | District | 2.5 weeks |
| 4 | Provincial | 2.5 weeks |
The design of the field attachment in its present form (one seven week block in the 3rd year of study only), is thus the product of a gradual evolutionary process over time. This was intended to overcome the curriculum challenges, of fragmentation and duplication of some objectives, as well as to minimise the economic challenges particularly in transporting students and conducting academic supervisory visits to the countrywide centres for each part of the four year programme.
The new design relies heavily on local supervisors to ensure that all objectives are covered and covered well. The quality of supervision of a rationalised programme design needed evaluation, in order to determine the feasibility of the demands being made on the local supervisors. Use of student perceptions is important because they are the recipients of education and as such, are an important group of stakeholders (11).
AIM OF THE STUDY
To evaluate physiotherapy and occupational therapy students’ experiences of the quality of supervision of the field attachment.
OBJECTIVES
- To rate the quality of supervision of the field attachment for the seven field attachment objectives as reported by students.
- To compare the students’ rating of the quality of the field attachment supervision with each of the following variables:
- Programme
- Year of placement
- Supervisor
- To determine the supervisor’s level of critical analysis of student’s performance on field attachment.
- To rate the social and emotional support and encouragement received by students during their field attachment.
METHOD
The survey was conducted at the University of Zimbabwe, College of Health Sciences in the Rehabilitation Department between 2004 and 2007. A 4 - year longitudinal survey of students’ perceptions of their experience of supervision of the field attachment was investigated by direct questionnaire.
All students registered for the third year of training for the Bachelor of Science Honours degree in Physiotherapy, or Bachelor of Science Honours degree in Occupational therapy for the years 2004 to 2007 at the University of Zimbabwe, were included in the study.
A researcher-designed questionnaire was used to gather data from students. The instrument profiled participant demographics, field attachment variables, methods and frequency of supervision and rated the quality of supervision for each attachment objective.
The quality rating was measured on a likert-type scale. Each broad objective of the field attachment was rated separately. An eighth item - social and emotional support and encouragement was included for rating. Although this is not an objective of the field attachment, supervisors are given this responsibility and it has previously been reported as an area of concern(10).
The objectives and eighth item were scored and rated separately. Thus, a total score of 32 could be obtained. Table 2 shows the ratings obtained therefrom:
| Description | Score | Rating | Percentage (%) |
|---|---|---|---|
| Outstanding | 4 | 25 ? 32 | >75 ? 100 |
| Good | 3 | 17 ? 24 | >50 ? 75 |
| Unsatisfactory | 2 | 9 - 16 | >25 ? 50 |
| Poor | 1 | 8 and 8< | 0 ? 25 |
The development of the questionnaire was influenced by the set objectives of the field attachment and the literature. It was piloted on 10 4th year PT and OT students in 2003, and was found to have content validity. The results of the pilot study were not included in the analysis of data of the main study.
Routine preparatory seminars (objectives, supervision and evaluation) for the field attachment were given two days prior to students departing for the field attachment. A pre-prepared handout was given to each student containing the content of the field attachment preparation.
One day after the students returned from the attachment, a peer evaluation session was facilitated by the principal investigator with each group. Immediately after this session students were introduced to the purpose of the study. Verbal consent was sought and obtained and the questionnaire administered to individual students. Students completed the questionnaire whilst the researcher observed that each student reported their experiences independently. Questionnaires were collected immediately, for all participating students after this process in February 2004, February 2005, February 2006 and February 2007.
Finally a measure of each student’s performance (local supervisors mark, presentation mark, peer rating mark and field attachment average) was entered onto a database.
Data Analysis
Data was entered into EpiInfo 2002. Descriptive statistics were generated to characterise the field attachment placements, describe the profile of the study participants and the frequency and methods of supervision.
A modal score was calculated for the quality rating of each objective, as well as for the item on emotional support and variability, calculated in terms of the inter quartile range.
Non ? parametric tests were used to calculate the differences between the modal score of comparable groups as follows:
- Mann Whitney - U test for the OT and PT students;
- Kruskal Wallis test. for:
- the four field attachment years
- the supervisor (PT, OT or Rehabilitation Technician)
Spearman’s rank correlation was calculated at the 0.05 level of significance for the:
- Field attachment average and supervisor’s mark.
- Field attachment average and presentation mark (the presentation mark was considered to be the bench mark and most objective, because it is determined by three independent adjudicators in the presence of an academic audience and places high demands on students to present an analytical overview of the attachment).
・The supervisors mark and the presentation mark were then regressed against the field attachment average. - Total quality rating score and the local supervisors mark.
- Total quality rating score and the field attachment average.
RESULTS
A total of 108 (100%) students participated in the study, 54 PT students and 54 OT students. The distribution of students by year was:
2004 ? 34 students (31.5%)
2005 ? 25 students (23.1%)
2006 ? 21 students (19.4%)
2007 ? 28 students (25.9%)
Students had been attached in districts in seven of the country’s ten provinces over the years. Table 3 shows the trend in attachment sites over the study period.
| Year of placement | Manical and 250-400km | Mash* central80-250km | Mash*East75-150km | Mash*West100-200km | Masvingo 300-450km | Mat† North600-900km | Midlands 250-450km |
|---|---|---|---|---|---|---|---|
| 2004 | 4 | 0 | 6 | 6 | 2 | 6 | 10 |
| 2005 | 2 | 4 | 5 | 2 | 4 | 0 | 5 |
| 2006 | 4 | 1 | 8 | 2 | 0 | 0 | 3 |
| 2007 | 0 | 4 | 17 | 7 | 0 | 0 | 0 |
| Total | 10(9.8%) | 9(8.8%) | 36(35.3%) | 17(16.7%) | 6(5.9%) | 6(5.9%) | 18(17.6%) |
Note: n = 103 (some students did not indicate their attachment site) *Mash ? Mashonaland, †Mat ? Matebeleland
The more distant provincial attachment sites have had fewer or no students in recent years.
The majority of students (60.2%) were supervised by a therapist (PT or OT), whilst 39.8% were supervised by a Rehabilitation Technician (RT).
Frequency and Method of Supervision
Over eighty percent (83.7%) of RT’s were considered to offer constant supervision as opposed to 46.2% of therapists (p<0.01).
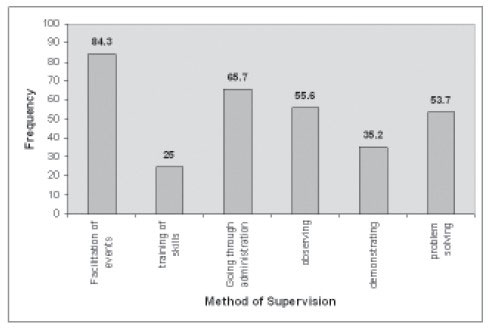
Figure 1 . Frequency of Methods of Supervision
{kind=link}
“Facilitation of events” was the most frequently cited method of supervision by 84.3% of respondents, whilst “training of skills” was the least cited by 25%.
Supervision of Objectives
Therapists and rehabilitation technicians were rated similarly on all objectives save for the objectives, on community involvement and CBR. Rehabilitation Technicians were rated better on supervision of the community involvement objective with 30% being rated outstanding vs. 6% of therapist supervisors (P<0.01). On the CBR objective, 37% of rehabilitation technician supervisors were rated outstanding vs. 8% of therapist supervisors (p=0.015)
Students from 2007 rated all the objectives lower than the previous three years, whilst year 2005 rated all objectives higher overall as shown in Table 4.
| 1. Demographic and social survey |
2. Conditions needing rehabilitation |
3. Organisation of heath and rehabilitation services |
4. Community involvement |
5.CBR | 6. Managing a rehab department |
7. Roles of staff |
8. Emotional support |
|
|---|---|---|---|---|---|---|---|---|
| 2004 | 3(2,3) | 3(2,3) | 3(2,3) | 3(2,3) | 3(2,3) | 3(2,3) | 3(3,4) | 3(3,4) |
| 2005 | 3(3,3) | 3(3,3) | 4(3,4) | 2(2,3) | 2(2,3) | 4(3,4) | 4(3,4) | 4(3,4) |
| 2006 | 3(3,3) | 3(3,3) | 3(2,3) | 3(2,4) | 3(2,4) | 3(3,3) | 3(3,4) | 4(3,4) |
| 2007 | 2(2,3) | 2(2,3) | 2(2,2.5) | 2(2,3) | 2(2,3) | 3(2,3) | 3(2,3) | 4(3,4) |
| p-value | not sig. | P=0.013 | P<0.01 | not sig. | not sig. | P<0.01 | p<0.01 | not sig. |
All values = Mode (IQR)
Over the four years studied, item eight - emotional support and encouragement was rated consistently good to outstanding.
None of the objectives was rated significantly different by PT students and OT students.
Total Quality Rating (TQR)
The modal total quality rating over the four years was 20 (62.5%) IQR = 17 (53.1%) ? 22 (68.8%).
The PT students gave a modal TQR score of 19 (59.4%); IQR = 16 (50%) -21 (65.6%) which was significantly lower than OT students who gave 20 (62.5%); IQR = 18.5(57.8%) ? 23.5 (73.4%), (p=0.03).
TQR was also statistically different among the four years, 2004 mode 20 (62.5%) (IQR=18 (56.2%) ? 21 (65.6%), 2005 mode 16 (50%) (IQR=19 (59.4%) ? 24 (75%), 2006 mode 19 (59.4%) (IQR=19 (59.4%) ? 23 (71.9%) and 2007 mode 16 (50%) (IQR=14 (43.8%) ? 20 (62.5%), (p<0.01).
Although RT supervisors obtained a higher modal TQR 19 (59.4%); IQR=18 (56.2%) ? 23 (71.9%), TQR was not significantly different between them and therapist supervisors 19 (59.4%); IQR =18 (56.2%) - 22.5 (70.3%).
TQR was also significantly different among frequency of supervision, with constant supervisors having a higher modal TQR 20 (62.5%); IQR=18 (56.2%) ? 23.5 (73.4%) than supervisors who supervised intermittently 20, IQR=18 (56.2%) ? 21 (65.6%) or rarely 10 (31.2%), IQR=11(34.4%) ? 14 (43.8), (p<0.01).
The student’s final field mark was positively correlated to the student’s TQR, Spearman’s correlation coefficient 0.156 (SE=0.072), (p=0.04).
Critical Analysis of Student Field Attachment Performance by Supervisor
The field attachment average was positively correlated to the supervisor’s mark, Spearman’s correlation coefficient 0.54 (SE=0.106) (p<0.01). However, the supervisor’s mark overrated student performance as it contributed great variance to the field attachment average (r2 =0.49) as compared to the variance contributed by the group presentation mark Spearman’s correlation coefficient 0.522 (SE=0.128) and (r2 =0.38) (p<0.01).
DISCUSSION
A total quality rating of 62.5% (good) was recorded for supervision of the physiotherapy and occupational therapy student’s field attachment at the University of Zimbabwe (UZ). Various social, environmental, academic and experiential factors are attributed to this finding.
A high rating for supervision was associated with constant supervision, the year 2005 and OT students tended to rate their supervisors more highly than PT students.
Other authors have previously reported student’s appreciation for constant supervision, which too has been the finding in this study (7,10). This may suggest the students’ need for constant guidance for community based learning and or in undergraduate learning. The community based teaching is not a routine approach in undergraduate health science programmes at the UZ, and it is possible that supervisors who themselves are graduates of the UZ programmes, lack the specific skills for community based teaching approaches. Whereas an increase in anxiety if supervision was given constantly so as to mimic spoon-feeding was reported (8), this element may be negated by the group nature of the attachment studied here.
A range of possibilities may account for OT students rating supervision more highly than PT students. The psychosocial focus of OT training may influence OT students to engender a more understanding nature when appraising the role of their supervisors. Alternatively, OT students may have a better predisposition to community based learning, thereby having less demands on the supervisor and subsequently rating them more favourably.
The good supervisor ratings by students from the year 2005 can be explained by the fact that it was in this year that the UZ academic department had a good staff complement. This, combined with a supportive faculty administration enabled 100% support follow up visits to attachment sites for the first time in many years. These events were timely in that, after rationalisation of the field attachment in 2004, the teething problems of 2004 were able to be addressed.
Subsequent attachment groups conducted their field attachment in an environment that was on a decline in many respects and came to be known as the economic melt-down in Zimbabwe (13). This was characterised by such socio-economic challenges as a high inflation rate, liquid fuel scarcity and thus transport non-availability, power and water supply interruptions, hence services and trade irregularity. Although these events had become evident prior to 2005, the escalation around this time became unbearable. The net effect of these occurrences that is immediately relevant to this study was the frustration of health professionals and the resultant mass exodus from the public sector, as well as from the country (14). In short the UZ had difficulty in finding supervisors for the field attachment. The few who held posts, were unwilling to take on student supervision duties, whilst those who were cajoled or coerced into student supervision had little or no resources to assist students to fulfil the attachment objectives. Chief among these was transport. Transport and communication has been cited as a significant barrier to supervision (10).
Attrition of Rehabilitation Technicians (a lower cadre providing rehabilitation services, also known as PT / OT assistant elsewhere) has been marginal over the years. Although they are employed across the health system, their training was designed as a stop gap measure at independence (1980), to provide rehabilitation services in the absence of PTs and OT s. The focus of their training was for community based services while based at the district level. Most of the RT’s are found at district level, and they have tended to serve their districts for longer periods of time. The higher quality rating for RT’s in their supervision of the objectives on community involvement and CBR, are indicative of their background training and long experience in community work. They are thus well established and familiar with the structures, protocols and community development strategies. The field attachment programme would do well to recognise this advantage and capitalise upon it in order to enhance the learning experience for PT and OT students on field attachment.
The low frequency reported in “training of skills” as a method of supervision, raises concerns. It may in part, be because a clinical load is not a primary objective of this attachment or that supervisors lack the experience, or do not engage in continuing education and subsequently lack the confidence to “train skills” or to “demonstrate” (10).
Critical Analysis of Supervisors
This study has revealed that supervisors tend to overrate student performance on field attachment. This unfavourable finding may be attributed to the confidence levels especially where an RT is required to supervise a therapist student. Supervisors may lack confidence in supervising students and in evaluating them, as they may fear that a low mark given to a student may reflect their own inadequacies as a supervisor, rather than reflecting student performance.
Social and emotional support and encouragement were rated consistently good to outstanding, this despite the challenging environment described earlier. This finding is highly commendable as it implied that supervisors were able to respond appropriately in this aspect of their supervisory role from both a personal, social as well as professional work perspective.
There may be diminished ability by professionals to respond in this manner when challenged and demotivated, particularly if they work in isolation, or outlying areas where collegial support is rare or absent. In this instance however, the finding may support the idea that the social fabric of small, rural and district communities is strengthened in the face of adversity.
CONCLUSION
Supervision of the field attachment has been rated “good” by PT and OT students. A constant type of supervision was rated highly for the undergraduate field attachment, with OT students having a propensity to rating their supervisors more favourably.
Rehabilitation Technicians were rated “outstanding” for their supervision of the field attachment objectives on community involvement and CBR. However, all supervisors overrated student performance on the field attachment.
RECOMMENDATIONS
Strengthening of the field attachment can be achieved through the continued training and support of local supervisors from the UZ.
All supervisors need to be trained on a) Methods of supervision, b) Frequency of supervision, c) Evaluation of students.
Therapist supervisors need training on supervision of CBR.
RT supervisors need training on supervision of identification and assessment of health and rehabilitation services.
The College of Health Sciences administration should continue to provide resources to enable academic staff to conduct follow-up support and supervisory visits.
Attachment placement of mixed OT and PT students should be continued.
The weighting of the field attachment evaluation components need to be reviewed.
* Senior Lecturer
Kigali Health Institute
P.O Box 3286, KIGALI, Rwanda
Tel: +250 03755608, Email : vyvienne2006@yahoo.co.uk
ACKNOWLEDGEMENT
The authors would like to acknowledge the participation of third year Occupational therapy and Physiotherapy students from the University of Zimbabwe (2004 - 2007). Also, thanks to colleagues past and present, from the Department of Rehabilitation, University of Zimbabwe who over the years designed and supervised the field attachment programme. The contribution of rehabilitation staff at district and provincial health facilities country wide, who supervised students, and the support they have had from their District Health Executives and Provincial Health Executives year after year, is also recognised.
Last but not least the authors acknowledge the administrative support the programme has received from the College of Health Sciences University of Zimbabwe through the Dean’s Office and the Field Attachments Office.
REFERENCES
- Heine D, Bennet N. Student Perceptions of level 1 field work supervision. Occupational Therapy in Health Care. 2003; Vol 17 (2): 89 ? 97.
- Gassner S. Community based prevention, management and treatment of HIV/AIDS 2006. Available at www.galilcol.ac.il/page accessed 1 November 2007.
- Fleshman M. Africa Agenda Items: Progress in Zimbabwe’s HIV/AIDS battle. African Renewal 2005 Volume 19(4): 3 available from www.un.org/ecosocdev/geninfor/afrec accessed 1 November 2007.
- Maponga C, Singairira A, Feresu BA. A community based clinical pharmacy teaching research and service programme in Zimbabwe. Pharmacotherapy. 1995. 15 (5): 614-620.
- Pipas CF, Carney PA, Eliasson MS, Mengshol SC, Fall LH, Russel K, et al. Development of a handheld computer documentary system to enhance ambulatory primary clerkship. Academic Medicine 2002. Vol 77: 600-604.
- Andrew S, Mckenzie B. Post Graduate research supervision: the student’s viewpoint. AARE Conference: Freemantle 2-6 December 2001.
- Dolmans DHJM, Wolfhagen IHAP, Essed GGM, Scherpbier AJJA, van der Vleuten CPM. The impacts of supervision, patient mix and numbers of students on the effectiveness of clinical rotations. Academic Medicine 2002. Vol 77: 332-335.
- Armstrong SJ. Impact of supervisor’s cognitive styles on the quality of research supervision in the management education. British Journal of Educational psychology 2004 Vol 74 (4): 599- 616.
- Taukobong NP. Community based clinical programme: The MEDUNSA Physiotherapy students’ experience. South African Journal of Physiotherapy 2004 Vol 60 (1): 7 ? 10
- Petrik M, Sichangwa K, Collinson M and Pickford K. Supervision of qualified community rehabilitation workers. South African Journal of Physiotherapy 2001 Vol 57 (1): 13 ? 19
- Dolmans DHJM, Wolfhagen IHAP, Scherpbier AJJA, van der Vleuten CPM. Relationship of tutors’ group dynamics skills to their performance ratings in problem based learning. Academic Medicine 2001 Vol 76 (5): 473-476.
- University of Zimbabwe Information Office. University of Zimbabwe Calendar/General Academic Regulations. University of Zimbabwe Publications. 2001 (Available from University of Zimbabwe P.O. Box MP 167 Mt Pleasant Harare, Zimbabwe)
- Confederation of Zimbabwe Industries.. Report on Manufacturing Industries in Zimbabwe. Financial Gazette Zimbabwe 2006. (Available from P.O. Box 66070, Harare, Zimbabwe).
- Herald Reporter. Shortage of Physiotherapists Hits Zimbabwe. The Herald, October 1, 2007. (Available from P.O. Box 396 Harare, Zimbabwe).
“DISABILITY & DEAFNESS IN THE MIDDLE EAST,
A BIBLIOGRAPHY”
http://cirrie.buffalo.edu/bibliography/mideast/index.html (also in pdf format)
First web published in 2002, and now revised and extended in 2008 with 70%
more items listed, and further annotation comprising materials with technical, cultural
and historical relevance to child and adult impairments, disabilities and
deafness, incapacity, mental disorders, special needs, social and
educational responses and rehabilitation.
This updated bibliography now lists c. 1750 items. It aims to record the cumulative
formal knowledge base in the disability field in countries of the Middle East, especially
Egypt, Iran, Iraq, Israel, Jordan, Lebanon, Saudi Arabia, Syria, Turkey, and some
smaller neighbours. Around 45% of the items in the bibliography, listed in the last
two sections with a brief introduction, comprise historical materials of the Middle
East from 1751 to 1970 and from Antiquity to 1750, as an essential and
fascinating part of the cultural background. Greater coverage has also been given to
disability and deafness in Egyptology, Assyriology, and the Hittite Kingdom in
Anatolia.