Field Visit Notes(*1)
8 September 1995
Government Institute of Rehabilitation Medicine, K.K. Nagar, Madras
The Government Institute of Rehabilitation Medicine at K.K. Nagar, Madras, is a premier rehabilitation and training institute. It is under the administrative control of the Director of Medical Education, Government of Tamilnadu.
Catering to persons with locomotor impairment, it is the only government institute in Tamilnadu which gives in-patient and out-patient care and conducts various rehabilitation training courses for professionals medical doctors, physiotherapists as well as orthotic and prosthetic engineers. The centre offers comprehensive rehabilitation through its various departments.
With a 40-bed in-patient facility, it caters, on an average, to about 250 out-patients per day. The Artificial Limb Centre at K.K. Nagar, Madras, is the only government manufacturing centre in Tamil Nadu. The mobility devices are given to patients at subsidized rates.
WORTH Trust, Katpadi
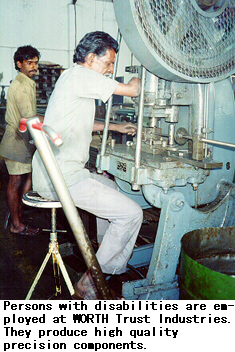
Worth Trust, a non-governmental organization registered as a charitable trust, works in various spheres of rehabilitation. It was established in 1963, in Katpadi, Tamil Nadu. Its engineering workshop provides employment to leprosy-cured persons and persons with other types of disability. The following are Worth Trust activities for people with disabilities:
- Transitional school;
- Vocational training centre;
- Production workshops in light engineering and plastics;
- Aids and appliances development centre and mobility aids unit;
- Orthopaedic workshop;
- Outreach programme.
In addition, it is in the process of establishing a rehabilitation training resource centre.
WORTH Trust has received grants from the government and private donors for capital expenditure and for establishing these centres. Once established, the centres do not depend on any outside support. Thus the two production centres develop enough resources to support the costs of running the transitional school and the technical training centre. A similarly self-sustaining complex has been established in two other towns of South India. Together, they constitute a good model for provision of rehabilitation services in developing countries.
The Katpadi production centre has thus far delivered thousands of wheelchairs and three-wheelers for the use of disabled persons. Many different models of wheelchairs and three-wheelers are being developed at the aids and appliances development centre. They represent improvements in design, leading to lowering of cost, efficiency of operation and reduction of maintenance requirements.

Worth-Perkins Brailler

The Worth-Perkins Brailler project is an example of efficient international cooperation between rehabilitation organizations in three different countries. It is also a successful model of an industrial venture which employs persons with disabilities to produce assistive devices and is financially profitable.
1. How did Worth Trust become involved in brailler production?
As an institution providing training and employment to persons with disabilities, WORTH Trust has been for many years producing mobility devices. The Christoffel Blinden Mission (CBM) has been an active WORTH Trust partner in the Trust's outreach programme.
CBM assists institutions for blind persons all over the world by donating braillers. They found that quality braillers were not available in India. Importing them often meant long delays and fulfilling cumbersome government regulations. The imported braillers were so expensive that they were beyond the means of most persons with visual impairments.
When Mr. P.G. Michael, the CBM representative for South Asia, Mr. Muggenburg of CBM head office in Bensheim, Mr. Gleason and Mrs. McPhillips from Perkins met at a conference in Germany, they agreed that the cost had to be reduced, if more blind persons were to benefit. Mr. Michael mobilized WORTH Trust interest in this project.
A study revealed that the cost could be substantially reduced by producing the braillers in India. The proposal to progressively manufacture the braillers locally received the wholehearted support of the Perkins, CBM and WORTH Trust Boards. CBM offered financial subsidy and the assurance of a minimum offtake of braillers. Perkins responded with financial and technical support. For WORTH Trust, it was within its technical capability to establish this unit.
2. What is the estimated demand for braillers in India?
The real demand for braillers is not known. In the past one year, five hundred WORTH Perkins braillers have been sold in India. Others who might buy braillers are not aware of its availability. Schools badly need them, but are dependent on government grants, which are difficult to process. The integrated education scheme, if implemented all over the country, may need a thousand braillers every year, depending on the implementation. So the demand is at least one thousand immediately and about five hundred every year. The brailler fulfills such a basic need that at least every student who is in high school must own one. It is not the demand that is limiting the sales but the ability to purchase.
3. What are the sources of the components used in its production?
For the first lot of five hundred, all the components were imported from Perkins. The next stage involves substituting the components with locally made ones. Many of the brailler components can be produced locally. To produce the components by injection moulding or pressure die casting, moulds are needed. These moulds are expensive to produce and maintain and unless sufficient quantities are produced, costs cannot be reduced through local production.
The raw material for the production of components is locally available or can be procured, if quantities of production justify the cost of development. To keep costs down, it may be advantageous to produce some and import others.
4. How many braillers does WORTH Trust plan to produce?
In the one year since production started, five hundred braillers have been sold in India, and another five hundred exported to the U.S. With the present capacity, WORTH can produce about 2000 braillers per annum. If there is a demand, the capacity can easily be increased.
WORTH Trust products for persons with visual impairments:(*)
- * Source: Antony Samy, WORTH Trust
5. Are people with disabilities involved in any aspect of production? If so, what type of accommodation has been made in the work place? What type of training have they had to perform their tasks?
Except for one person, the entire workforce of ten, including three women, consists of persons with disabilities. The one visually disabled person does inspection and also works on the assembly. The building is accessible in every way, with wide ramps up to the second floor, and sufficient aisle space, so that persons using wheelchairs can move about comfortably. The work benches are built to facilitate easy assembly. Two of the workers hold technical certificates. They and the others, who had only high school education, had no prior exposure to any industry.
6. For other workers, what was the duration and type of training?
The training is on-the-job and is usually for two years, during which time, they are fully involved in production. Two experts from Perkins were with WORTH Trust twice for short periods, providing training in assembly and testing. The Manager and his assistant received two months training at the collaborators' facilities in the U.S. Four workers also received three months of intensive training in the U.S.
7. What is the purchase price of the WORTH-Perkins brailler? Is the production a profitable venture for WORTH Trust?
An imported brailler cost almost Rs. 30,000 (US$ 850). With local assembly, the price came down and, with a subsidy made available through Perkins, the price was drastically reduced to Rs. 9500 (US$ 270) in India and US$ 375 for export. As WORTH Trust was established to assist persons with disabilities, production is not pursued as a profit-making activity. WORTH Trust provides some services which are not fully charged. The unit generates marginal surplus. When production increases, even with all costs, the venture will continue to be financially self-sustaining.
8. What are the channels for marketing and distributing the brailler?
The braillers are marketed directly by WORTH. They are also sold through national and international associations for blind persons and in Germany through a non-profit organization.
9. Does WORTH Trust plan to export the brailler? If so, where to and what is the status of the export plans?
WORTH-assembled braillers have been tested and approved by an independent expert in Germany. After this, bulk exports have been made to an organization in Germany and, through that organization, to other countries. The braillers have been exported to Bangladesh, Nepal and USA. Recently, orders have been received for Kenya and Uganda, where the braillers will be field-tested.
10. Additional information
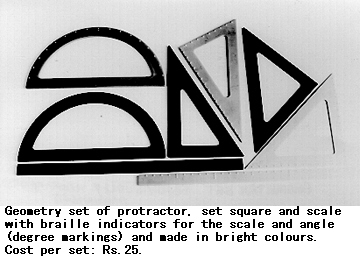
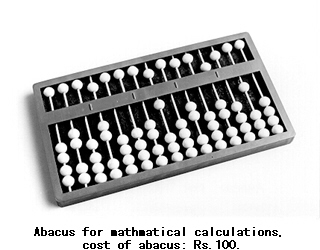
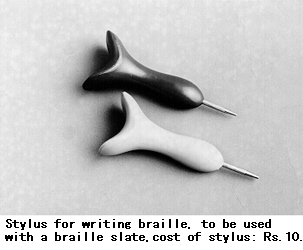
WORTH Trust also produces a stylus to international standard and markets this. Geometric instruments and the abacus for the use of persons with visual impairments are under development.
WORTH Trust Production of Wheelchairs, Tricycles and Adapted Motorcycles


WORTH Trust regularly produces different models of wheelchairs and three-wheelers to fulfil individual orders. Many are improved versions of other designs.
WORTH Trust embarked on wheelchair production over 30 years ago. Initially, by working with local users to incorporate their feedback, foreign models were adapted to suit local conditions and meet local user needs. The people who made the wheelchairs were technicians who had no formal diplomas.
When Mr. Ralf Hotchkiss visited WORTH Trust, its foreman, Mr. Natarajan, supervised the production of the "Hotchkiss" model wheelchair for demonstration purposes. Mr. Natarajan has a diploma in mechanical engineering. Like other co-workers in the WORTH Trust team, he had had no practical training or experience in wheelchair production prior to working at WORTH Trust.
The technicians acquired their skills after joining WORTH Trust. Some, like Mr. Natarajan, also had the opportunity to make short visits abroad as part of the WORTH Trust development programme.
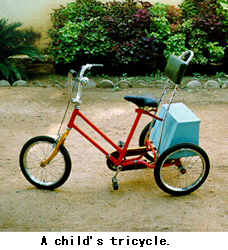
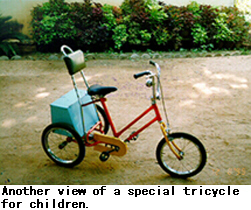
WORTH Trust tricycles
1. Details of the WORTH Trust best-selling models of tricycles
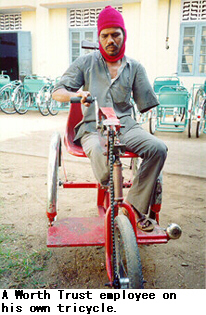
WORTH Trust started producing tricycles for the use of its trainees and employees who needed them. The design emphasis was on low cost, minimum and easy local maintenance possibility, and ruggedness to suit the local terrain. There was good demand. Subsequently, thousands of the basic model were sold to the public and distributed through government procurement. WORTH Trust encouraged others to produce the tricycles by providing training and technical information. Through the years, while minor improvements were incorporated, the basic model remained the same.
(a) Market prices:
The exfactory prices of three- wheelers are:
| Indian Rupees | US$ | |
| Friendship model for children with cushion seat and back | 2900/- | 83 |
| Friendship model for children with carrier box | 3000/- | 86 |
| Friendship model for adult with metal seat and back | 3100/- | 89 |
| Friendship model for adult with cushion seat and back | 3400/- | 97 |
(Packing and forwarding charges are extra.)
(b) Marketing and distribution channels in India
The tricycles are sold directly from the WORTH workshop and despatched to destinations all over India.
(c) Production capacity
Although WORTH Trust has produced more that 1500 in a year, the present capacity of the mobility aids unit is 1000 three-wheelers. It produces far fewer for want of orders. The capacity can easily be increased to even 2000 units per year.
(d) Research and development aspects of the WORTH Trust tricycle programme
Although the rugged model was accepted by most people, it was realized that a wider choice had to be provided.
First, two sizes of three-wheelers were produced. Realising the deficiency of the original models, a more efficient one was developed in collaboration with the Centre for International Cooperation and Appropriate Technology (CICAT) of the Delft University of Technology, Netherlands, and in cooperation with two non-governmental organizations producing mobility devices in Sri Lanka (Sarvodaya Wheelchair Workshop, Ambalangoda) and Thailand (McKean Rehabilitation Centre, Chiang Mai). It was field-tested in these three countries. Based on field-test experiences it was redesigned and standardized as the "Friendship" model. It is made in two sizes, for adults and for children. This is WORTH's best-selling model.
(e) How easy or difficult is it for users not living in the vicinity of WORTH Trust outlets to obtain spare parts and services for repair and maintenance?
The three-wheeler is used all over the State of Tamil Nadu and beyond its borders, so it is not practical to bring it back to the factory for repairs.
All the components used in this tricycle are standard cycle components, which are easily available even in small cycle shops in rural areas. Furthermore, the three-wheeler is built in such a way that it can be easily repaired and maintained using simple tools.
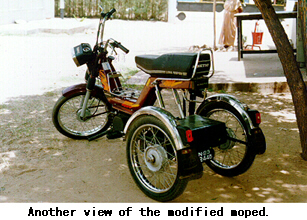
2. Background information on commercially available tricycles and adapted motorcycles in India
There is a wide range of three-wheelers commercially available; most are produced by organizations for disabled persons. Until recently, motorised three-wheelers were custom-built and each small-scale producer used his/her own design, often altering it to fulfill the needs of individual customers. With the glut in the moped/scooter market, these vehicles are more easily available. Many persons with disabilities now buy these vehicles, add two more wheels for stability and use them. But these vehicles are not practical for those who use wheelchairs. For them, no standard model is available.
Range of market prices
The price of tricycles in the market may vary between Rs. 2,500 to Rs. 3,500 depending on the producer and selling pattern.
In the case of a three-wheeler fitted with a diesel/petrol engine, the price may vary between Rs. 10,000 for an ordinary locally fabricated one and Rs. 30,000 or more, for an altered moped or scooter.
9 September 1995
Department of Physical Medicine and Rehabilitation, Christian Medical College (CMC) and Hospital, Vellore

Vellore is situated 150 km. south-west of Madras; it is easily accessible by rail or road. The station for those travelling by broad gauge lines is Katpadi, 7 km. from Vellore Cantonment. Regular bus services operate through Vellore from Madras and Bangalore.
The Christian Medical College (CMC) and Hospital was founded by Dr. Ida Scudder, the daughter of a missionary medical doctor. Realizing the need for women doctors in India, Ida Scudder obtained her medical training in the United States and returned to India to help her father with his work. It was in 1890 that Dr. Scudder started her work, using one room for in-patients in her father's bungalow. Patients flocked to her hospital in ever increasing numbers and the need for providing more beds and better facilities was soon apparent. Dr. Scudder set about winning support and sympathy for her cause. In 1902, the Mary Taber Schell Hospital was built with accommodation for 40 patients. In 1924, the present hospital site was acquired and a 267-bed hospital was built. Today, there are 1,766 beds for in-patients; nearly 2,300 out-patients are treated daily. The doctors, nurses, para-medical workers and non-medical teachers come from nearly every state in India as well as from Australia, Canada, New Zealand, U.K. and U.S.A.
Extensions of the hospital include an eye hospital, a mental health centre, two rural hospitals (CHAD & RUSHA), a rehabilitation institute for disabled persons who require prolonged treatment and training. There is also a college of nursing (affiliated to the Tamil Nadu Dr. M.G.R. Medical University) offering both undergraduate and postgraduate courses.
Situated 5 km. from the main hospital, the college campus is set in a 200-acre site. The grey granite buildings of the college and chapel date back to 1932. Part of the non-clinical teaching is carried out at the College. The students attend hospital for clinical work and the rest of the courses. The College is now supported by 81 churches and missionary societies in India and abroad and is administered by a Governing Council in India consisting of their representatives.
At the Christian Medical College and Hospital, the treatment and rehabilitation of patients with many kinds of disabilities is the coordinated effort of a number of departments and specialists, including doctors, nurses, physical, occupational and speech therapists, social workers and vocational traininers.
All available expertise is utilized to enable those with physical and mental disabilities to fulfil their potential, helping each to find his/her rightful place in society, with opportunities for all to become contributing members of their families and communities.
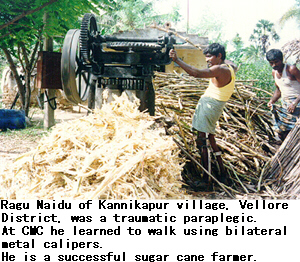
Started in 1966 by Dr. Mary Verghese, herself paraplegic, CMC's was the first residential medical rehabilitation centre in India. Twenty-nine physically disabled patients can be accommodated for long-term therapy, training in activities of daily living and suitable vocational training.
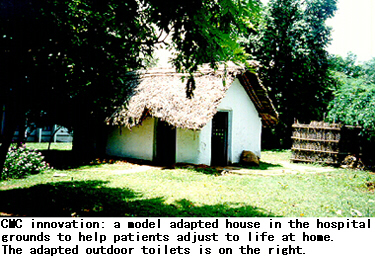
Many of the patients spend a week or two in a model hut in the centre where their home situation is simulated as far as possible. Here they carry out activities of daily living where their independence is gauged. A workshop facility within the main hospital, the Artificial Limb Centre, makes custom-fitted appliances, equipment and footwear for patients, as needed.
11 September 1995
Schieffelin Leprosy Research and Training Centre (SLR & TC), Karigiri


The Schieffelin Leprosy Research and Training Centre, Karigiri, is situated about 140 kms. from Madras and is close to the well-known Christian Medical College and Hospital, Vellore. This institution was established 40 years ago, in 1955, both to take care of persons with leprosy, as well as to study the disease and find answers to the complex medical and social problems it causes. It has 200 beds for in-patients and a field area of about 70,000 population for leprosy control activities. This institution has, over the years, accomplished pioneering work. In Gudiyatham Taluk alone which is assigned to the Centre by the Government, over 25,000 patients have been treated; the prevalence has been reduced from 26 patients per 1,000, to 1 patient per 1,000 population.
About 20,000 reconstructive and other related operative procedures have been performed. Hospitalization facilities have been enhanced. The Centre now caters to about 2,500 in-patients and over 35,000 out-patients every year. Additionally, relevant work is carried out in rehabilitation aspects, eye care, medical management, and laboratory diagnosis. Karigiri is renowned internationally for the quality of the training offered to professionals in the field of leprosy. Through the efforts of many committed workers, who carry out their tasks with diligence and zeal, as well as the financial support of many like-minded funding bodies, this institution has grown from strength to strength.
The Centre's pioneering work in assistive devices include the following:
- Invention of a rubber that compensates for loss of plantar subcutaneous tissue, popularly known as micro cellular rubber (MCR).
- Karigiri models of foot wear for insensitive feet.
- Orthopaedic shoes for various foot deformities.
- Splinting for therapeutic activities and managing the activities of daily living.
- Assistive devices for partially sighted and blind leprosy patients.
- Assistive devices for the management of extensive deformity in leprosy patients.
11 September 1995
Rural camp for fitting artificial limbs: The MUKTI approach(*3)

MUKTI is a unit of the M.S. Dadha Foundation. It was established by Meena Dadha in Madras in 1986 to provide artificial limbs to physically disabled persons. In this, it received technical assistance from the Bhagwan Mahaveer Viklang Sahayata Samiti of Jaipur. For its caliper production, MUKTI adopted the methods used by ADD-MOBILE, Bangalore. Individuals and social service clubs, such as the Rotary, Round Table, Jaycees, and Lions, contribute in cash and kind to MUKTI's fulfilment of its mission. The Government of Tamil Nadu contributed the land for MUKTI's premises.
MUKTI has adapted modern technology and used new materials to develop lighter, more durable and easily affordable artificial limbs. These limbs, made of high density polyethylene, enable poor peasants to run, jump, climb, walk on uneven ground, pedal, squat, sit cross-legged and work in the fields. Fitting of the limbs is free or at a nominal cost.
To extend its service to the rural poor, MUKTI conducts an extension programme which includes holding camps to fit limbs. Normally camps are conducted for eight days (Sunday to Sunday). Approximately 60 limbs can be made in that period of time.
The costs involved include the following: average rate of Rs. 500 per day, expenses for the travel, board and lodging of five technicians, and the incidental expenses incurred in running the camp. Also included are charges for hiring equipment and the transport costs for bringing raw materials to the site.
The requirements for conducting a camp are:
- The space required is three rooms: one for measuring and fitting, another for producing, and a third for the technicians to sleep in, as they tend to work late into the night. In addition, there should be enough space for amputees to wait and rest.
- Running water and electricity are also required. The assistance of someone with orthopaedic skills and a medical doctor would be advantageous.
- The services of two local volunteers (who need not have prior knowledge of how to make prostheses) to assist in limb production would facilitate the work. Another helper would be needed to maintain cleanliness. A fourth helper would be needed to manage the amputees, make executive decisions and maintain sponsor's accounts and other paper work.
Local newspapers in the vernacular language spread information about a camp that is due to be organized. MUKTI also uses posters for awareness raising.
A MUKTI camp is usually organized as follows:
- Day 1: The technician checks all amputees to ascertain whether limbs may be fitted. In the case of those who can receive limbs, measurements are taken and moulds made on the first day.
- Days 2 and 3: The technician works on the limbs.
From the afternoon of Day 4 onwards, fitting will be carried out in a phased manner. Training will be provided on the use and care of the limbs.
The provision of each limb costs MUKTI Rs. 1,430. For a camp organizer, the cost of sponsorship of an artificial leg is Rs. 750. The sponsorship charges of artificial hands are Rs. 2,000 per hand (capable of activity, but is not cosmetic).
Generally, a limb lasts about three years, although much depends on how it is used. Disabled persons from Nepal, Sri Lanka, as well as the Andaman and Nicobar Islands are among the users of MUKTI limbs.
In its sponsorship programme, MUKTI offers to industrialists and industrial concerns the option of sponsoring an annual camp to provide MUKTI limbs to orthopaedically disabled persons in the villages surrounding the respective industrial establishment. MUKTI also encourages the employment of suitably qualified persons who have received the limbs. In another option, an annual commitment is made between MUKTI and the industrialists or industrial concerns whereby orthopaedically disabled persons are periodically sent to MUKTI in small groups. During the three to four days that it takes for the fitting, a representative from the nearby branch of the sponsoring industry or organization makes the arrangements for their stay.
12 September 1995
Gandhi Rural Rehabilitation Centre (GRRC), Alampoondi
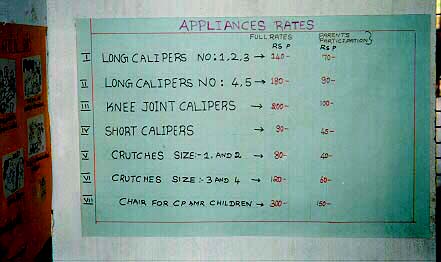
The Gandhi Rural Rehabilitation Centre (GRRC) is a NGO which started in 1983 to create employment for physically disabled people. The workshop employs about 60 workers, (the majority of whom are disabled) in weaving, tailoring and embroidery. This unit is self-supporting.
GRRC runs a polio treatment centre. The administration of this unit is partly entrusted to the parents of the polio-affected children. When a child is brought in for treatment, the parents are requested to become members of the parents' association. This association meets once a month and decides the main orientation of the centre. Parents pay Rs. 5 per month. The treatment consists of training the parents in how to address the needs of their disabled child and to help with the necessary exercises. If required, the child is provided with crutches and/or calipers made out of PVC pipes. The advantage of using PVC material is that it is locally available, low-cost and light in weight. A child with weak muscles finds it difficult to use heavy calipers. Since the child is growing, she/he will need to change her/his calipers every year. The PVC material is strong enough to last one year. The parents meet about 50 per cent of the expenses of the material. The crutches and calipers are made in a workshop attached to the polio centre.

During one of their meetings, the parents requested GRRC to open a hostel for polio-affected children. This was started in Aniladi and attached to a junior high school. There 25 children study in classes from first to 10th standard. Parents meet about 25 per cent of the expenses of the hostel. Selection for admission into the hostel is by a committee. The parents have a major role in the committee. Rules for admission have been decided by the parents.
Recently, at the request of the parents of children with intellectual disabilities, a new day-care centre was opened. It looks after 10 children. Here again, the policy was to involve parents from the planning stage. Several meetings were held with them before they were requested to give their suggestions and help. Since the centre is runing with limited resources, once fortnightly, the mother of each child comes to help the two teachers. Apart from the help given to the centre, it is an opportunity for every mother to learn how to bring out the best in her own child at home. This day-care centre is situated in a beautiful garden where GRRC has a social forestry programme. It gives opportunity to the intellectually disabled children to work in the nursery and to be in close contact with plants and trees.
The main thrust of GRRC work is to answer needs expressed by the local community, with the maximum involvement of the local people and minimum input from outside of the local community.
The GRRC received considerable technical guidance from the Rehabilitation of the Disabled in India (RDI). RDI is the local body representing Handicap International in India Below is further information on RDI's genesis, philosophy, multipurpose rehabilitation technicians and technology project.


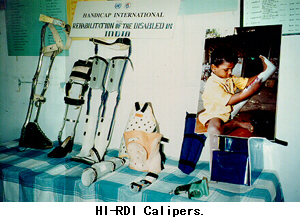

Rehabilitation of the Disabled in India (RDI)
Genesis and Philosophy
At the request of a local association in Pondicherry called CERTH India, an orthopaedic workshop was established in 1988 by Handicap International. In view of the high incidence of anterior poliomyelitis, it was decided to start a pilot project for the treatment and appliance fitting of children presenting post-polio residual paralysis.
The objective of this project was to add another option to the existing system in India for the delivery of orthotic appliances, which would address the needs of those without access to the existing services.
The constraints of the existing system are among the reasons for the high rejection rate for orthosis among disabled children. In the usual procedure to prescribe orthotic appliances, the client has to be assessed by a physiotherapist who tests his/her muscle power; then a specialist in orthopaedic surgery is consulted who decides the type of appliance the person needs. Finally, the device is made by an orthotist. The decision for fitting is often taken by looking only at the results of muscular testing, without considering the functional abilities of the child.
The disabled person's point of view and feeling regarding what she/he needs is seldom considered by the decision-makers, who view the disabled person as a medical case rather than as a person.
The choice of appliance should be made by technicians with basic knowledge of physiotherapy; the users should be involved in taking the decision, so that there is greater acceptance on the part of the user.
For many children affected by poliomyelitis, calipers are necessary to prevent deformities. Furthermore, the appliance, should also improve, or at least preserve, the ability to move. Prescription must be based on a balanced choice between the possibilities of functional improvement and the requirements of prevention. The system developed at Pondicherry was a response to existing constraints in giving independent mobility to persons with disability.
Rehabilitation of the Disabled in India (RDI) was registered in 1993. RDI is in partnership with 20 organizations in southern India to train and support personnel for the management of rural orthotic workshops.
More than just the technology, RDI shares a philosophy with its partners and tries to evolve a system which considers the basic needs of children with disabilities as a whole, so as to enable them to play an active role in the community. This approach does not interfere with the existing network of professionals whose targets are most often at other levels, in city-based structures and in making private practice.
Multipurpose Rehabilitation Technician (MRT)
The multipurpose rehabilitation technician (MRT) trained by RDI in Pondicherry is a technician for calipers, as well as a physical therapy assistant and an animator. Such technicians working at the field level are in a position to decide about therapy and fitting for most of their clients without depending on the specialist's decision.
The role of the MRT includes:
- Assessing the needs of the child with polio;
- Organizing the child's physical rehabilitation care;
- Establishing rapport with and ensuring the cooperation of parents;
- Choosing the appropriate appliance;
- Producing the appliance;
- Training the child to walk and balance with the appliance;
- Organizing technical and medical follow-up.
The fitting of an appliance is sometimes just a temporary way of learning how to adapt to the disability. The orthotic support required by a young child who has never walked before is different from what is needed by a teenager whose bones have attained full growth. For a small child, the focus may be more on prevention of further problems, but fitting should be as light as possible to improve ability to move and to facilitate acquisition of new skills in daily life.
The needs of the child with a disability must be assessed at regular intervals, as he/she keeps changing, growing and improving his/her abilities when given a proper chance. Basic physiotherapy exercises can be provided by the parents, with monitoring by community rehabilitation workers and regular follow-up assessment by the MRTs, focusing on the long-term needs of the child.
The physiotherapy helps to:
- Prevent and correct contractures;
- Prepare the child for caliper fitting;
- Teach the correct use of the assistive device;
- Strengthen partially weakened muscles;
- Help the child adjust to the disability.
When evaluating the child's needs for physical therapy and for assistive devices, the MRT must keep in mind the objective of integrating the child into the community. Hence, one aspect to be given major importance in the process of rehabilitation is community involvement. The best persons to implement basic treatment and follow-up are the child's parents and relatives.
Community support should address the family's need for basic help to carry out rehabilitation at home. A key challenge is to develop understanding in the community regarding what disability is and to foster positive attitudes towards persons with disabilities. To achieve rehabilitation, equal opportunities must be given to persons with disabilities to fulfil their role in society. In this, the positive attitude of MRTs as well as other field workers is essential, as they have to serve as advisors and facilitators with regard to the community, and the disabled persons and their families.
Issues
The following are some problems related to the availability of assistive devices and obstacles in the proper delivery of services in the present system:
- The prescription and delivery of assistive devices depend on the willingness and availability of a series of professionals forming the compulsory official channel.
- The cost of the assistive device is high, compared to the resources of the communities concerned.
- The heavy weight of the metal orthoses discourages wide use.
- The orthopaedic leather shoes are not appropriate for the tropical climate and the rural context, and are difficult to manufacture and maintain.
- The few workshops which are accessible to rural communities, face many constraints related to high demand, manufacture time, and availability of materials, all of which result in long waiting lists.
Technology
The RDI project developed a type of orthotic equipment made out of thermoformable plastic material easily available in the Indian market.
- Rigid PVC is used in the manufacture of drain pipes.
- Polypropylene is a flexible plastic used in the making of many products such as furniture and containers. It can be bought in the form of industrial sheets.
Advantages
The technicians' calipers suit well the orthopaedic requirements for prevention, functional adaptation and, in some cases, correction of deformities.
The channel from prescription to delivery depends on one technician, who is trained as a physiotherapist assistant, along with the person with a disability.
The cost involved is one-third cheaper than the cost of conventional calipers. For example, the price of a long caliper, according to the child's age, varies from Rs. 120 to Rs. 250.
It is washable, and enables the user to wear ordinary types of sandals or shoes.
It is more popular with children because of its light weight
It is easy to manufacture in any small assembly workshop, using prefabricated components delivered by centrally-based production workshops. Hence, a permanent stock of standard models, in different sizes, can be adapted to the needs of each disabled child.
It takes a short time to manufacture. A short caliper can be made in two hours; a long caliper in half a day.
13 September 1995
Rural Camp at Tiruporur (Organized by District Rehabilitation Centre, Chengelput)
The District Rehabilitation Centre (DRC), Chengelput, is one of the 11 DRCs funded by the Ministry of Welfare, Government of India. It is administered by the Directorate for the Rehabilitation of the Disabled, Government of Tamil Nadu.
The DRC-Chengelput, housed in the campus of Chengelput Medical College, covers in phases the various blocks of the District of Chengelput.
An assessment clinic was conducted at the village of Alathur by DRC-Chengelput. The village Alathur is located on the eastern side, 1 km. from Mahabalipuram Tiruporur Road Junction, which is 10 km. from Mahabalipuram. The population of the village is 1,550. The assessment clinic was conducted by the specialists of the District Rehabilitation Centre, Chengel- put.
About 50-60 disabled persons from adjoining villages, i.e. Alathur, Pyayannur and Cothavakkam, attended the assessment clinic.
The clinic assessment focused on:
- Type and degree of disability;
- Medical and surgical needs;
- Need for assistive devices;
- Educational needs;
- Vocational needs;
- Social needs;
- Therapeutic needs.
The District Rehabilitation Centre Scheme
The District Rehabilitation Centre (DRC) Scheme of the Ministry of Welfare, Government of India, was started in 1985. Its aim was to provide total rehabilitation services at the door step of the persons with disabilities in rural areas, through a 3-tier system of community-based service delivery following a systems approach and utilizing multipurpose rehabilitation functionaries recruited and trained at community level.

As it was envisaged that establishing linkages with services already existing in the community would make the scheme more cost effective, the second tier personnel was abolished in 1990.
The Government of India started the DRC Scheme to offer a lead role to the State Governments in India to address the fact that only less then 2 percent of persons with disabilities had been rehabilitated; that too, where 90 percent of the services were located in urban areas, while 70 per cent of people lived in rural India.
The awakening created by the International year of the Disabled Persons (IYDP) in 1981 and the launching of the IMPACT International Programme at New Delhi in 1982 clearly brought the following to the forefront:
- Services are grossly inadequate.
- Appropriate services are not available to rural disabled persons.
- Poverty, illiteracy, ignorance and supersition prevalent among the rural masses are factors that add to the sufferings of disabled persons and make a disability into a handicap.
- Disability rehabilitation involves a lengthy process.
- Shortage of trained manpower for rural rehabilitation compounds existing problems.
Establishment of the National Institutes for the Hearing Handicapped, Visually Handicapped, Mentally Handicapped, Orthopaedically Handicapped and the DRC Scheme were the major initiatives to circumvent the above issues through governmental initiatives, involving the NGOs wherever possible.

Today, there are 11 District Rehabilitation Centres in the country supported by four Regional Rehabilitation Training Centres offering training, material development, R & D and technical inputs. The Central Administrative and Co-ordination Unit (CACU), New Delhi, with a Project Director at the rank of Deputy Secretary to the Government of India, is funding and monitoring the entire Scheme.
The National Institutes for Hearing Handicapped (Bombay), Mentally Handicapped (Secunderabad), Visually Handicapped (Dehra Dun), Orthopaedically Handicapped (Calcutta), and the National Institute of Rehabilitation, Training and Research (Cuttack), along with lead NGOs in the country, in addition to the National Institute for Disability Rehabilitation & Research, Washington DC, are involved in strengthening and updating the DRC Scheme.
Modus Operandi
At village level, there is one anganwadi Worker (AWW) for every 1000 population under the Integrated Child Development Scheme (ICDS) of the Government of India. The AWW is trained for 72 days in a job training course. The ICDS Scheme is being implemented by the State Governments. The AWW is additionally trained for 12 hours in Disability Prevention and Management by the Regional Rehabilitation Training Centres of the DRC Scheme. She will identify children and adults with disabilities through door-to-door surveys, create awareness in the community, refer the needy to the assessment clinics conducted by the DRC in each cluster of villages, undertake follow-up services in terms of recommendations and use of aids and appliances, and report the felt needs of disabled persons/families.
The District-level team has fully qualified professionals such as:
- Physiotherapist;
- Occupational therapist;
- Speech therapist and audiologist;
- Orthotic and prosthetic engineer;
- Ear mould technician;
- Social worker.
The team will conduct clinics along with PHC doctors. The District Rehabilitation Officer who is heading the DRC is a District-level Senior Administrator of the State Government, who will plan and execute services for disabled persons. The services available at the DRC are:
1. Medical/surgical treatment through referral to the State Health department.
2. Audiological assessment.
3. Fitment of aids/appliances and accessories, eg., ear mould mak- ing.
4. Physiotherapy, occupational therapy and speech therapy.
5. Arranging school admissions, scholarships, and loans.
6. Arranging vocational training, and placement.
7. Guidance and counselling.
8. Coordination of prevention activities, along with the Health Department.
The DRC depends on the ICDS network, parent training programmes and local NGOs for continued therapy provision.
The largest number of disabled persons served under one scheme is the DRC Scheme. More than 1,200,000 persons have benefitted so far.
The Government of India has plans to expand the scheme to all the districts in a revised plan. This is to be achieved in a phased manner in the Eighth and Ninth plan period, ending in 1997 and 2002, respectively. Empowering persons with disabilities, and local bodies through the Panchayat Raj Act is a new thrust to provide equal opportunities to persons with disabilities.
Regional Rehabilitation Training Centres (RRTCs)
The four RRTCs situated in four regions of the country are the training and research wings of the DRC Scheme and its 11 DRCs.
The training faculty of each RRTC consists of 5 Master Trainers with the rank of Assistant Professor in (a) rehabilitation medicine; (b) physio/occupational therapy; (c) speech therapy and audiology; (d) prosthetic and orthotic engineering; (e) social work/vocational counselling/psychology.
Functions of RRTCs
1. Training
(a) Provision of orientation training for DRC professionals and training of multipurpose rehabilitation functionaries of the DRC Scheme, doctors and health personnel of the Health Departments, revenue officials, bank officers, industrialists, teachers and village leaders to augment service delivery through the DRC Scheme;
(b) Training of anganwadi workers, supervisors and instructors of the ICDS Scheme;
(c) Training of allied health professionals/personnel of various courses recognized by the Rehabilitation Council of India conducted by government agencies and NGOs.
2. Material development
(a) Preparation of training manuals and course syllabi for all the above training programmes;
(b) Preparation of awareness and media materials for public education;
(c) Preparation of identification checklists, referral and follow-up slips for service delivery.
3. Research
Undertake research on:
(a) Development of appropriate and cost-effective technology;
(b) Delivery of appropriate rehabilitation services;
(c) Training of rehabilitation functionaries.
RRTC, Madras, provides umbrella coverage to the three southern DRCs of Chengleput in Tamil Nadu, Mysore in Karnataka, and Vijayawada in Andhra Pradesh, besides covering the ICDS training programmes of these three States, Kerala and the Union Territory of Lakshadweep and Pondicherry. Located in the K.K. Nagar Government Institute of Rehabilitation Medicine (GIRM), both RRTC, Madras, and GIRM, Madras, utilize each other's infrastructure and personnel for training and other purposes. The Head of the Government Institute of Rehabilitation Medicine is the Honorary Regional Director of RRTC, Madras.
*1 Based on information provided by the Government of India for the reference of participants, to facilitate their observations in the field visit segment of the Technical Workshop on the Indigenous Production and Distribution of Assistive Devices, and on details gathered in the course of the field visit.
*2 Antony Samy, Managing Director, Worth Trust.
Antony Samy, a U.S.-trained engineer has devoted 35 years of his life to help build WORTH Trust into the success story it is today. When he began his work at Katpadi, people affected by leprosy were thrown out of their homes and had no source of livelihood. No one wanted to touch any thing made by leprosy-affected persons. From such beginnings in an under-developed area, grew two thriving production centres for light engineering and electronics. The centres support WORTH Trust's social service programmes for the rural poor.
*3 A limb of utility is a joy forever, MUKTI brochure; and MUKTI's Artificial Limb Camps, MUKTI leaflet which is sent to prospective camp sponsors.
Photographs:
1. WORTH Trust products for persons with visual impairments:


2.Worth Trust tricycles & motorcycles









Indigenous Production and
Distribution of Assistive Devices:
Some Critical Issues
Below are notes prepared by the participants as background information to the recommendations of the Workshop. In view of the expertise available among the participants and the emphasis of the Workshop on devices for persons with mobility difficulties, there is greater focus on persons with spinal cord injury.
1. Poverty of disability data and information
There is a need for adequate data on disability. Without it, it is difficult to develop plans and programmes for rehabilitation services, the production and distribution of assistive devices, and related training. These are essential means of enabling persons with disabilities to live meaningful and productive lives in the community.
The majority of persons with disabilities in ESCAP developing countries live in the rural areas. They are poor and have little awareness or information concerning available rehabilitation services and assistive devices. To meet their needs, appropriate assistive devices have to be produced and distributed, especially in the rural areas.
2. Poor coordination, insufficient training and inadequate follow-up
The problem is compounded by lack of coordination among producers, NGOs, and concerned government agencies, with attendant problems of duplication and wastage. While it is commendable that high technology and standardization has occurred in some countries of the region, however, a lack of trainers and training programmes for the indigenous production and distribution of assistive devices is a major issue in most developing countries of the region. Follow-up services for users remain a high priority which is yet to be addressed.
3. Persons with spinal cord injury (SCI)
Spinal cord injury (SCI) usually results from an accident that breaks or severely damages the central nerve cord in the neck or back, falls from trees or donkeys, traffic accidents, diving accidents, bullet wounds, and other injuries. Spinal cord injury of the neck causes tetraplegia (quadriplegia) in which all four limbs are affected. Injuries of the back cause paraplegia, in which only the lower body and legs are affected.
Spinal cord injury is on the ascent due to increasing numbers of traffic and industrial accidents, as well as violence and armed conflict. As most accidents involve young and active members of the community, if proper rehabilitation services are not provided and persons with SCI remain dependent on their families and community, the loss to society is enormous.
When the cord is damaged, feeling and movement in the body below the level of the injury are lost or reduced. In most developing countries of the ESCAP region, many persons with SCI do not survive because of the medical conditions associated with spinal cord injury. Those conditions include pressure sores and other injuries on the paralysed part of the body, as well as bladder and kidney (urinary) infections. Severe mental depression also causes many such persons to consider or commit suicide.
The lack of knowledge among medical professionals about the treatment and rehabilitation of persons with SCI, as well as proper locomotor and self-care devices, prevent the full participation of persons with SCI in community activities.
The training of medical professionals and health workers, to increase their knowledge and skills concerning the rehabilitation of persons with SCI is important, in order to prevent the occurrence of dangerous medical complications.
Due to the loss of movement of the lower limbs, most persons with SCI use wheelchairs. However, in many cases, a person with injury in the lower back can walk with leg braces and crutches.
As the mobility of most persons with SCI is extensively impaired, progress in the production and availability of low-cost and high-quality locomotor devices is essential (e.g., wheelchairs, tricycles and light weight braces). Wheelchairs are one of the most expensive assistive devices. There is great need for the development of low-cost and locally-adapted wheelchairs. Also essential are low-cost cushions for pressure sore prevention, as well as devices and techniques for bladder and bowel control.
Persons with SCI often develop new ways of sensing and interpreting the needs and functions of their bodies. The best persons to help newly-injured individuals learn those subtle signs and the know-how to respond to them are experienced persons with SCI.
Many persons with SCI experience phases of deep depression and helplessness when they feel unable to accept their disability and move forward with their lives. Peer counselling by persons who have had the same experience and have successfully re-integrated into society is one of the most effective approaches to helping this group emerge from the difficult periods of depression.
Experienced peers play an important role in encouraging the use of appropriate devices for a more active life. Promotion of leisure and sports activities for persons with SCI can help to lift their spirits, maintain their physical health, and encourage social integration.
In recent years, positive efforts have been made in ESCAP developing countries for the rehabilitation of persons with SCI. In the Centre for the Rehabilitation of the Paralysed (CRP), near Dhaka, comprehensive services are provided for and, to a large extent by, persons with SCI. CRP produces medical and rehabilitation equipment as well as assistive devices, including wheelchairs, trolleys and walkers with locally available materials. It employs former patients as counsellors for new admissions. CRP provides literacy training and extensive vocational training for persons with SCI. Many of the trainers are themselves disabled.
The Rehabilitation Institute for Disabled Persons, Christian Medical College and Hospital, Vellore, Tamil Nadu, India, provides comprehensive rehabilitation services for persons with SCI. One of the major features of the Institute is the choice it gives persons with SCI, through training, to walk with braces and crutches. This is because the use of a wheelchair is usually not feasible in the rural environment.
There are many breakthrough in the technologies for both prosthetics and orthotics, which make the devices cheaper, easier to make and more comfortable or functional. However many of these technologies are not yet in wide use. It is often the smaller, more innovative community programmes that are using them, while the larger programmes and institutions are still using older and more costly, but less satisfactory, production methods.
There is, therefore, a need for more exchange among programmes, whereby those using newer and more appropriate methods can help other programmes in setting up or modifying their production workshops. The use of plastics in the making of orthopaedic appliances is an area of great need for technical cooperation.
4. Persons with multiple disabilities, especially cerebral palsy (CP)
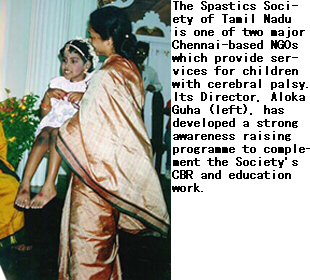
In most Asian and Pacific developing countries, the problems faced by persons with multiple disabilities, including those with cerebral palsy (CP) are more difficult than those faced by persons with other types of disabilities. There is poor awareness, even among professionals, about the situation, needs and aspirations of this group.
There are few programmes which are inclusive of persons with CP and few services for them. Existing ones are mostly in urban areas. There is a need for basic training of community workers in the provision of rehabilitation services for persons with CP in the rural areas.
Persons with CP face considerable problems in participating in family and community life. Equalization of opportunities for their participation is minimal. The problems are rooted in a common belief that having a child with CP is a punishment from God or retribution for past misdeeds. Thus, families tend to hide their children with CP at home without proper rehabilitation services, education and the other learning experiences that all children are entitled to.
The rehabilitation of persons with CP is a lengthy and intensive process compared with the rehabilitation of persons with other types of disabilities. It requires a multidisciplinary approach.
5. Persons with visual impairments
It is estimated that the population of persons with extensive visual impairments in the 15 countries represented in the Workshop could be about 28 million. The majority are estimated to be in Bangladesh, China, India, Indonesia and Pakistan. The number of people with low vision in these countries is approximately 90 million. They can all benefit from the provision of assistive devices.
In 1981, WHO held its first meeting on the use of residual vision. It produced recommendations and definitions for practice and service in the field of low vision. Since then, there have been a number of developments. New resource materials have been produced for training, and there is an increase in the manufacture of assistive devices for persons with visual impairments.
Many countries now have low vision centres. The concept of low vision is now increasingly understood in terms of behavioral function rather than on a medical basis. The majority of people with visual impairment have some vision. According to a variety of surveys, among children in special schools for the blind, 30 to 40 per cent have vision that could be used in daily activity. However, children in developing countries are rarely encouraged to develop the use of that residual vision and its existence is often ignored by medical and educational staff. The challenge during the Asian and Pacific Decade of Disabled Persons is to identify ways of enabling partially-sighted people to benefit from their remaining vision through the provision of appropriate services, training, materials and devices.
The causes of low vision in developing and developed countries differ. The biggest single cause of visual impairment in developing countries is cataract, followed by corneal opacities (caused by trachoma or other eye infections plus trauma), glaucoma, diabetes, and retinal and neural disorders. Most of the causes are preventable and curable. A multi-disciplinary and integrated approach is required involving doctors, primary health care workers, community rehabilitation workers, optometrists, opticians, special education teachers and, most of all, people with visual impairments themselves.
It is a matter of concern that, in many developing countries of the region, the important area of low vision devices has been grossly underdeveloped. It is only in recent years that scattered efforts have been made to address the problems of low vision. Many countries are now producing simple low vision devices and other devices for blind persons. Some are producing more sophisticated devices, e.g., closed circuit television systems. Some countries are meeting the need for assistive devices with local resources. Others are dependent on the import of those devices from countries within and outside the ESCAP region.
Special and integrated schools for blind and low vision children exist in most countries of the region. However, their number does not suffice to meet the needs of both groups. Most special schools are located in cities, while the rural population, which forms about 70 per cent of the total population, has no access to those facilities. Furthermore, there are too few vocational training institutes and trained personnel. The institutes usually do not have access to advanced methods of training in the education of children with special needs.
CBR programmes for the rehabilitation of people with visual impairments are among the efforts made in the past few years to address the above-mentioned problems. More countries now have low-vision programmes. In some countries, the integration of persons with visual impairments into mainstream society is promoted through a policy of reservation or special quota in Government and public sector jobs.
6. Persons with hearing impairments
The magnitude of speech and hearing impairment is difficult to assess. Perhaps suitable production strategies shall offer commercial viability. The know-how for commercial production of hearing aids is available within the ESCAP region.
Emphasis needs to be given to prescription and training infrastructure. Countries in the region with the expertise concerning techniques and devices relating to hearing impairment could make known the nature of the expertise and the focal point for inter-country contact.
In developing countries of the region, experience indicates that if hearing aids are well maintained through proper care, it is possible to use them for well over 12 years. It is also noted that the cords of hearing aids break faster in the tropics.
Go back to the Contents
ECONOMIC AND SOCIAL COMMISSION FOR ASIA AND THE PACIFIC
Production and distribution of assistive devices for people with disabilities: Part 2
- ANNEX 1&2 -
ST/ESCAP/1774
UNITED NATIONS PUBLICATION
Sales No. E.98.II.F.7
Copyright © United Nations 1997
ISBN: 92-1-119775-9