MYANMAR *
* By Mr. Thaung Shwe, Assistant Director, Department of Social Welfare, Yangon.
The Ministry of Health set up community-based rehabilitation (CBR) pilot projects in selected areas through the sample survey on people with disabilities. All these projects have made marked progress in the promotion, implementation and evaluation of CBR, and have achieved good results. As a result of CBR, the Ministry of Health made arrangements for assistance by providing the assistive devices to people with disabilities in the community as well as in the hospitals. Furthermore, assistive devices for physically disabled persons are produced in the workshop under the Department of Health, with the support of NGOs and United Nations agencies. For persons with visual impairments, a CBR programme included manuals and training programmes for community volunteers to learn to identify disabilities and to provide simple assistance, white cane and low vision devices. To promote better education and work for the integration of the deaf people in the community, CBR deals with many programmes in the community and institutions.
In carrying out the preventive and rehabilitative measures for person with disabilities, assistive devices are major requirements of people with disabilities. Therefore, production and distribution of assistive devices are being arranged to provide the necessary assistive devices to disabled persons through CBR projects.
A. Need for assistive devices
There are no national statistics on the number of people with disabilities in the country, so the exact need for assistive devices cannot be defined at present.
The National Rehabilitation Hospital provides devices to those people with locomotor disabilities who are being given medical treatment as in-patients and out-patients. With the assessment of individual cases through early intervention and treatment, the Hospital decides whether devices are to be provided or not.
Through medical treatment programmes, assistive devices are produced in hospitals. Assistive devices, including wheelchairs, braces, crutches, walkers and artificial limbs, are made in hospital workshops. Those outside hospitals can receive devices through CBR services. People with disabilities in rural areas receive devices made in the community or in a hospital.
Under the arrangements of Prevention of Blindness programmes, efforts are being made to provide white canes and low-vision devices to people with visual impairments who are under treatment. To provide assistive devices for people with visual impairments, the Prevention of Blindness programme has requested low vision aids from World Vision International, the funding agency for the programme.
These devices are generally imported through funding agencies such as World Vision International. The most common devices imported include low vision aids and teaching aids such as braille. These materials are fully supported by the funding agency, World Vision International. The donating agency makes arrangements for customs clearance and custom duties with the coordination of the Health Department. There is no customs duty on these devices.
Some devices for people with locomotor disabilities are also imported, generally from donating agencies through CBR projects. More commonly imported are materials, such as epoxy resin and hardener, materials for soft insert, material for making calipers, and thermo plastic, or components, such as retainers, joint bolts and nuts or external knee joints. Clearance will be made by the donating agency or if it is destined for the Health Department, the latter will do so.
The Prevention of Blindness project provides medical treatment to people with hearing impairments in a community-based approach. Their rehabilitation is initiated by the Department of Social Welfare through an institution-based approach by two schools for deaf people.
The majority of assistive devices for people with locomotor disabilities in Myanmar are made of locally available materials, such as wood, leather and rubber.
Assistive devices for people with hearing impairments are arranged by personnel from hospitals and schools for deaf people. These devices are imported by two international NGOs. The main types of devices are audiometers and related devices, hearing aids and batteries. Indigenous and imported hearing aids are available, but there is no guarantee for the indigenous hearing aids. For most of this equipment, an import permit is needed, but if it comes under a health project, then only a minimum amount of customs duty must be paid by a funding agency.
B. Policy
The production and distribution of assistive devices is a major programme for people with locomotor disabilities. Through the national health plan and various projects such as CBR, necessary devices are produced to meet the needs of people with disabilities in urban and rural areas. According to the National Health policy, the required assistive devices are produced and distributed to people with disabilities.
The Health Department is carrying out the production and distribution of assistive devices for blind people through a pilot community-based approach. Under the project of Prevention of Blindness, standardization of assistive devices is controlled by the Health Department.
There are six programmes and 47 projects including projects for hearing impairments in Myanmar. There is no specific issue for standardization of these devices. Their standardization is controlled by the Health Department. Assistive devices for people with hearing impairments are provided in hospitals, special schools and communities.
C. Production capacity
It is difficult to estimate the number of devices produced per month, although production capacity in the country is expected to increase progressively with demand in the future.
Assistive devices for people with visual impairments are fully supported by World Vision International and Christoffel-Blinden Mission. Arrangements are under way to produce assistive devices for blind people in the near future, with the cooperation of the Department concerned.
Assistive devices for people with hearing impairment are supported by two international organizations. It is difficult to mention the number of production units of the assistive devices made locally.
Production capacity is limited for both financial and technical reasons. The financial limitation is in the case of devices needed, where reliance is mainly on imported components and materials. The technical limitation is in cases where there is a shortage of trained technicians.
D. Repair and maintenance
There are two workshops, run by the Health Department, for the repair and maintenance of assistive devices for people with locomotor disabilities. One is in Yangon, the other in Mandalay. The Mandalay workshop is mainly responsible for the repair of prostheses, while the Yangon workshop is responsible for all kinds of repairs including leather and rubber vulcanizing facilities.
There are no workshops for the repair and maintenance of assistive devices for people with visual or hearing impairments.
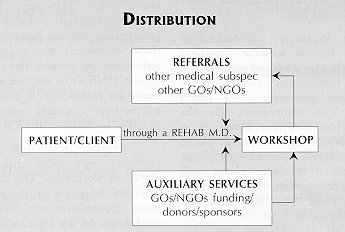
E. Distribution
Distribution of devices for people with locomotor disabilities occurs through institution-based centres. The service is available to all people with disabilities who are able to come to these centres. People with disabilities registered in the centres will be provided with appropriate assistive devices according to their socio-economic status.
Assistive devices are available to all people with visual and hearing impairments through various programmes. They must contact the nearest health centre for treatment and preventive programmes.
F. Technology
Prosthesis production is based on two types of technology: plastic-resin impregnation technology and polypropylene technology. For orthoses, production is based on metal, thermoplastic and leather technology. See Table 1 for a list of items and components made in Myanmar.
Assistive devices for people with visual and hearing impairments are mainly provided by NGOs.
G. Personnel
Assistive-device technicians are supervised by the Health Department in the production and distribution of the necessary devices for disabled persons who register in the National Rehabilitation Centre. These technicians include prosthetists-orthotists, and orthopaedic and brace makers among them; there are no technicians for assistive devices for people with visual or hearing impairments.
The training of the technicians is conducted at the National Rehabilitation Hospital which developed a curriculum. Certificate training and on-the-job training (apprenticeship schemes) are available to technicians. The technicians are all employed by the Government.
H. Institutional support
The Ministry of Health is the sole source of support for material and technology for assistive devices for people with locomotor disabilities, while the Ministry of Social Welfare, Relief and Resettlement is responsible for socio-economic support.
International NGOs, such as the International Committee for the Red Cross, World Vision International and the Advantaged Development Relief Agency (ADRA), provide support for imported components and sometimes for imported technology.
World Vision International and Christoffel-Blinden Mission are the funding agencies supporting people with visual impairments. Similarly, funding agencies such as World Vision support the indigenous production and distribution of assistive devices for people with hearing impairments.
I. Technical Cooperation
Myanmar is interested in participating in programmes of technical cooperation as both a donor and a beneficiary. As a beneficiary, it could use the following assistance and technology:
(a) For people with locomotor disabilities:
- i) Rubber foot production technology;
- ii) Production of much needed polypropylene raw material for prostheses fabrication;
- iii) Socket design technology.
(b) For people with visual impairments:
- i) Production of braillers, low-vision devices, white canes and educational devices.
(c) For people with hearing impairments:
- i) Audiologists;
- ii) Ear moulding;
- iii) Speech training;
- iv) Teacher training.
Table 1: National Rehabilitation Hospital Artificial Limb Workshop
1. Production of artificial limbs, braces and crutches
| Years | Artificial limbs | Braces | Crutches |
| 1992 | 376 | 310 | 940 |
| 1993 | 393 | 296 | 1185 |
| 1994 | 392 | 465 | 1000 |
|
2. Machines
|
3. Materials
|
NEPAL *
* By Ms. Shashi Kala Singh, Chairperson, Technical and Skill Development Centre for Blind and Disabled, Kathmandu.
A. Need for assistive devices
Written information and statistics on assistive devices could not be found in the bulletins and papers published by the Government, NGOs or the private sector in Nepal. As a result, this paper is prepared on the basis of discussions with different government officials and NGO personnel in the related fields.
The sample survey of 1982 indicated that three per cent of Nepal's people had disabilities; in 1992, the figure had reached 15 per cent of the total population (2,865,000). Currently, less than three per cent of their needs are being met. Nepal has not yet developed a system by which the majority of its disabled citizens has access to needed assistive devices.
Assistive devices are imported in limited numbers, purchased with the help of donor agencies and individual donors. Devices for people with locomotor disabilities, including artificial limbs and tricycles, are primarily imported from India. Assistive devices for blind persons and deaf persons, including braille materials and hearing aids, are generally imported from Germany, Japan and the United States of America.
Devices imported through institutions are subject to a one per cent duty. Devices imported by people with disabilities for their own use are subject to a minimum 10 per cent duty. If the devices are imported for business purposes, no duty is charged.
There is only small-scale production of assistive devices in Nepal. There is a need to develop and organize more larger-scale production of various types of assistive devices.
B. Policy
There is no explicit government policy in Nepal concerning the local production, import and distribution of assistive devices. There are no national standards for assistive devices either. There is no division in Nepal's national standards body that addresses standards for assistive devices.
C. Production capacity
The government-run Bir Hospital, NGOs and one private-sector organization are producing calipers, orthopaedic shoes, and wooden and bamboo crutches in limited numbers. Leprosy Hospitals (Kathmandu and Pokhara) and the Hospital and Rehabilitation Centre for Disabled Children (HRDC) are producing assistive devices for their patients. Orthopaedica, a private agency, produces orthopaedic shoes. The Disabled Relief Fund and the Disabled Children Rehabilitation Centre fund individuals to buy the devices.
The HRDC, Leprosy Hospitals, Bir Hospital and Orthopaedica only produce units for their individual patients. However, there are not enough units produced per month to meet those patients' needs.
The potential production capacity for orthopaedic shoes, calipers, braces, artificial limbs and crutches is estimated at 70-90 units per month. This capacity is limited both by financial and technical problems.
Neither any organization nor the Nepal government produce assistive devices for people with visual impairments, hearing impairments or cerebral palsy.
D. Repair and maintenance
The extent to which repair and maintenance services for assistive devices are available is not known.
E. Distribution
There are no mechanisms for distributing assistive devices in Nepal. To obtain devices, children below 15 years of age are referred to the HRDC, and leprosy patients can get devices from the Leprosy Hospitals. Other people with disabilities must find a donor agency or individual donor to support them and pay for the device to be made at a private workshop (Orthopaedica) or in India.
F. Technology
Electric hand tools are used in the production of assistive devices, although electrical free-standing machines are not. Drilling, wood carving, grinding, welding, lathe and mechanical equipment are also used. Knee joints, ankle joints, hip joints and uprights are the components made locally in Nepal. Local raw materials include leather and wood. Components made in India, including products of ALIMCO, are imported; the average unit cost is Rs. 900 (US$4.50).
G.Personnel
There are few trained assistive-device technicians in Nepal. Engineers from other fields, including machinists, welders and fitters, also make assistive devices. Training specifically for assistive devices usually occurs outside Nepal as no training is available in the country, except for a small orientation program held by HRDC for its CBR workers. This programme helps them identify the needs of people with disabilities who are in villages.
Of the assistive-device technicians in the country, four are self-employed, eight are employed by the Government and 14 are employed by NGOs.
The Technical and Skill Development Centre for the Blind and Disabled is interested in starting a programme that would train students to assemble wheelchair parts. This could help develop a cottage industry to repair and assemble wheelchairs, bicycles, and their components. A 1993 survey discovered that there was no technical expertise in Nepal to produce wheelchair parts. If the Centre could gain access to wheelchair parts, or the finances to purchase them, it could begin this programme.
H. Technical cooperation
Nepal does not have the trained personnel nor the finances to be able to contribute technical assistance, training or funding to the programme. It would, however, like to be a beneficiary of technical assistance, including training, programmes. Technical and training assistance is needed in the production of assistive devices for blind and deaf people and in large-scale production of assistive devices for people with locomotor disabilities and cerebral palsy.
PAKISTAN *
* By Dr. Hasan Minto, Co-ordinator, Principal Optometrist, Pakistan Institute of Ophthalmology, Visual Efficiency Research and Instructional Centre, Rawalpindi
This paper provides a review of the situation of people with all types of disabilities but, given the area of expertise of the author, it focuses on those with visual disabilities.
A. Need for assistive devices
No systematic survey has recently been conducted to estimate the number of people with disabilities in Pakistan. A World Health Organization (WHO) survey conducted in 1984, however, estimates that about 10 per cent of Pakistan's population, or about 12.5 million people, have disabilities. A small survey carried out in 1986 by the Directorate General, Special Education(DGSE), estimates that the prevalence of disabilities, in percentage terms, is:
| Locomotor disability | 34 |
| Mental disability | 22 |
| Multiple complex disability | 19 |
| Visual impairment | 15 |
| Hearing impairment | 10 |
B. Policy
The Directorate General of Special Education (DGSE), established in 1985, is responsible for the formulation, implementation and coordination of a national policy and programmes for people with disabilities. Major future programmes are:
- (a) Provision of low vision aids;
- (b) Establishment of special education centres at district headquarters;
- (c) Establishment of orthotic-prosthetic workshops;
- (d) Assembly of hearing aids:
- (e) A Regional Institute of Training and Research on Special Educa- tion.
C. Supply
This section of the paper discusses import policy, indigenous production capacity, institutions, technology and human resource issues. All the above issues are discussed separately for each major type of disability.
1. People with locomotor disabilities
It is estimated that over three million individuals in Pakistan have locomotor disabilities. The Government of Pakistan allows the import of motorized wheelchairs and special vehicles free of import duties and taxes. At present no figures are available on the total number of motorized wheelchairs and special vehicles imported, or their cash value.
Pakistan produces all prosthetic and orthotic devices indigenously and is able to meet the registered demand for these devices. However, many people with disabilities, especially in rural areas, are not identified and are not counted as part of the demand which is met.
Types of orthoses manufactured at present include:
- (a) Surgical boots;
- (b) Symes foot;
- (c) Collars;
- (d) Calipers;
- (e) RJSS spinal supports;
- (f) Telepiece splints;
- (g) Abduction splints;
- (h) Braces;
- (i) Corsets;
- (j) DB splints;
- (k) Abdominal belts;
- (l) Stock hand splints;
- (m) PTB belts;
- (n) Knee caps and T straps;
- (o) Brace joints.
Crutches and walkers are produced in all cities and major towns by local carpenters and metal workers. Wheelchairs and tricycles are produced by two bicycle factories in Pakistan. These devices are repaired by local technicians or the institutions that produce them.
There are about 10 institutions in the government and NGO sectors involved in the production of assistive devices. In addition to this, several small entrepreneurs produce assistive devices as a cottage industry.
Devices are manufactured using wood, plastic, leather, and stainless steel, which are easily available locally. Equipment used in producing the devices includes cutters, lathes, drill machines, copying lathes, carving machines, grinding machines and hand tools. All the equipment is operated manually.
The cost of prostheses in the government and NGO sectors ranges from US$10 for a simple orthosis to about US$100 for a full prosthetic limb. The prices in the private sector are much higher and are not regulated.
The Government provides full coverage for the provision of assistive devices to the poor. People with disabilities who require assistance can apply to National or Provincial Rehabilitation Centres and will receive all devices free of cost.
Although most technicians learn to make assistive devices through apprenticeship with an artisan, there are some formal training courses. Peshawar University offers a full four-year course leading to a bachelor's degree in prosthetics and orthotics. Polytechnic and vocational institutions offer courses in carpentry, machinist and metal work. Physiotherapy courses are offered at two universities in Pakistan.
2. People with mental disabilities
No special assistive devices are manufactured in Pakistan for people with mental disabilities. No information is available on the import of assistive devices to meet the needs of persons with such disabilities. However, if required, the Government of Pakistan allows duty-free import of any and all devices for disabled persons.
The Government and the NGO sector have a number of institutions providing educational and vocational rehabilitation training for persons with intellectual disabilities.
3. People with hearing impairments
The Government has provided facilities for audiological assessment at all District Hospitals in the country. The assessment is, however, conducted by ear/nose/throat specialists rather than trained audiologists. A programme to train the required number of audiologists is under way. Recently, the Ministry of Health, with the collaboration of WHO, has initiated a National Prevention of Deafness Programme.
At present, hearing aids are not produced in Pakistan; demand is met only through (duty-free) imports. The total volume of the import and its cash value cannot be estimated.
The National Institute of Electronics, under the Ministry of Science and Technology, has produced and tested a prototype hearing aid which conforms to international standards. Mass production of hearing aids is still to be initiated. However, hearing aid moulds are made in Pakistan at centres in Islamabad, Lahore, Karachi and Peshawar.
The Government provides hearing aids to children with hearing impairments free of cost, if an application is made to the national and provincial Centres for the Rehabilitation of the Disabled. There is no provision to supply free hearing aids to adults. The cost of an imported hearing aid ranges from US$50 to US$400.
All audiological assessment equipment is imported and there are no plans for its indigenous manufacture.
Speech therapy and other training for people with hearing impairments is being provided by a number of centres managed by the Government and NGOs.
4. People with visual disabilities
A national survey in 1987-1990 sponsored by the Ministry of Health and WHO claims that about 1.78 per cent of Pakistan's people are blind. About 2.4 million people are blind in both eyes. According to this survey, about 0.5 to 1 million people can benefit from assistive devices for people with low vision.
The four most common causes of blindness in Pakistan are cataract (67 per cent) corneal opacity (13 per cent), uncorrected refractive errors (11 per cent) and glaucoma (4 per cent). There are over 500,000 people who must be treated as blind because they have no glasses or other low-vision aids.
A national directory, published by the Directorate of Special Education, indicates that Pakistan has 60 centres for people with visual impairments, with a staff of 300 teachers. They provide education and rehabilitation to 3000 enrolled students. Most of these centres are government-run, with a significant contribution by NGOs to maintaining the rest. The rehabilitation offered in these schools is mainly in the use of braille and navigational methods. Low-vision aids have yet to be utilized.
The National Programme for Prevention of Blindness (1994-1998) has addressed this issue. There are 18 tertiary eye-care centres in the country. It is proposed that these centres work in close liaison with the centres for visually handicapped persons.
The national health policy makes special reference to the rehabilitation of people with disabilities. The Directorate of Special Education, and its apex training institution, the National Institute of Special Education, have shown tremendous concern for the development of low vision services in Pakistan.
The Al-Shifa Visual Efficiency Research and Instructional Centre was established in 1993. It began as a low-vision clinic to help those who could be helped with standard refraction; this clinic still operates weekly. The large numbers of poor people attending the clinic made it necessary to develop a process whereby they could be prescribed and dispensed locally manufactured low-vision aids. Furthermore, a study of three schools for blind people in Rawalpindi and Islamabad demonstrated that about 50 to 60 per cent of the children enrolled there could be helped with low-cost low-vision devices.
A research and development project undertaken by the Al-Shifa Centre has resulted in a wide range of affordable low-vision devices using locally available material and appropriate technology. The cost of these devices is low, from US$2 to US$20. The materials used in their production are optical glass, PVC pipes and plastic. The mode of production is manual, using lens surfacing generators, cutters, edges and grinders.
At this stage, an interim service that can utilize existing personnel and infrastructure is required. This would involve institutional strengthening and capacity building with human resources development over the next ten years. During this period, this specialized service should be integrated into the existing health services structure, and should become an integral component of all future national health policies relating to special education and the prevention of blindness.
At present, Pakistan has facilities for braille publication and copying, and conversion of computer text to braille text. In addition, full courses from the primary to the graduate level are available on audio cassettes. Recently, a newspaper has introduced a talking edition for blind people. Most centres for people with visual disabilities have these facilities.
To guide policy-making and to monitor development of an infrastructure for low vision services, a National Task Force has been formed.
In collaboration with the National Institute of Special Education, the Al-Shifa Centre is conducting courses in order to train low-vision therapists to prescribe low-vision devices and train patients in their use. Opticians are also being trained to produce low-vision devices locally.
Plan for Development of Low-Vision Services in Pakistan
|
NATIONAL PLAN FOR PREVENTION OF BLINDNESS COMPONENT FOR REHABILITATION OF THE VISUALLY HANDICAPPED |
||
|---|---|---|
| NATIONAL COMMITTEE FOR PREVENTION OF BLINDNESS | TASK FORCE FOR DEVELOPMENT OF LOW VISION SERVICES | MINISTRY OF SPECIALEDUCATION |
|
AL-SHIFA VISUAL EFFICIENCY RESEARCH ANDINSTRUCTIONAL CENTRE (ASVERIC) |
- | DIRECTORATE OF SPECIAL EDUCATION NISE |
Technical expertise, research and development of low-cost LVAs Training of trainers and opticians for LVAs Development of courses and educational material and toys |
- |
Coordination Manpower Development Administration Facilities for LV therapy Training of LV therapists at centres for visually handicapped persons |
| OPTICIANS | LOW VISION AIDS |
Other NGOs and other organizations |
|
TERTIARY EYE CARE CENTRES |
REHABILITATION | CENTRES FOR VISUALLY HANDICAPPED PERSONS |
| - | PATIENT REFERRAL |
LOW-VISION THERAPISTS |
D. Technical cooperation
In principle, the Government of Pakistan welcomes opportunities for technical cooperation in the region. Pakistan's Government and the institutions involved in providing services to people with disabilities will be more than willing to fulfill their responsibilities towards people with disabilities elsewhere in the region.
Pakistan has made significant advances in the field of low vision and is open to provide all possible facilities and technical expertise to its regional partners.
Pakistan is willing to explore and negotiate the role that it needs to play in regional cooperation. A role for Pakistan can be defined based on its strengths and weaknesses in the field relative to those of other partner countries.
Pakistan is committed to regional technical cooperation and resource sharing, and notes its responsibility to people with disabilities not only in Pakistan but in the whole region.
Orthotics and Prosthetics Centre
During the period of 1 July 1989 to 30 June 1990, 1269 people with disabilities were newly registered at the Orthotics and Prosthetics Centre. In addition, 97 repairs were made. The new registrations included 230 men, 141 women, 603 boys and 295 girls, for a total of 1269.
The number of produced and delivered units at the Orthotics and Prosthetics Centre is given below:
Orthotics and Prosthetics Centre
| Type of device | Produced | Delivered |
| Orthopaedic shoes | 820 | 817 |
| Braces | 364 | 365 |
| Abduction splints | 4 | 4 |
| Corsets | 190 | 188 |
| Cervical collar | 26 | 24 |
| DB splints | 238 | 227 |
| Prosthesis | 55 | 55 |
| Abdominal belts | 30 | 26 |
| Stock hand splints | 70 | 68 |
| PTB belts | 112 | 112 |
| Knee cap & T. straps | 640 | 605 |
| Brace joints | 2630 | 1820 |
| Prosthesis joints | 60 | 60 |
| Misc. | 175 | 175 |
| Total | 5314 | 4546 |
In addition to the above, 113 minor repairs were made. Concessions on 598 appliances/limbs worth 371,971 rupees were given to deserving patients.
PHILIPPINES *
* By Dr. Betty Dy-Mancao, Department of Rehabilitation Medicine, Philippine General Hospital, University of the Philippines, Manila.
A. Need for assistive devices
At present, the country is still in the process of getting reliable statistics regarding its people with disabilities. On 3 December 1995, a National Registration Day for the Disabled was held nationwide, to allow government agencies and NGOs working together to achieve the common goal of obtaining accurate and reliable statistics.
House-to-house surveys were performed for whole municipalities implementing the national Community-Based Rehabilitation Program (CBRP), indicating that between 6 and 7 per cent of the population had disabilities. At least 30 per cent of them would need assistive devices at some point.
Handicap International, an NGO that makes orthoses and prostheses, has established 15 workshops in the Philippines. Thirteen private workshops are located around the country, but are mainly located in the metropolitan areas. There are only four workshops for other assistive devices, primarily ambulation aids like canes, crutches, walkers, and wheelchairs. These devices are usually imported instead, bought from Germany and Taiwan, province of China. Materials used in prostheses are also imported from Germany and Taiwan, province of China.
Imported materials are subject to customs duties and tariffs. The Philippines has adopted the service of SGS (Societie General Surveillance) so that computation of customs duties is performed in the country of origin of the materials, making customs clearance easier in the Philippines.
Ambulation aids are mostly donated to people with disabilities. Prostheses, orthoses and orthopaedic shoes also used to be donated in large numbers. This practice, however, has been discouraged because these devices are highly user-specific and must custom-fit each user. Donated devices are still made use of by removing reusable components like the knee joint and shaft. The socket is then modified, or one is newly made to fit the user properly.
The need for ambulation aids has been met without great difficulty through the Community-Based Rehabilitation Program, because their manufacture is easily taught. Orthoses, prostheses, motorized wheelchairs and hearing aids, however, are more complicated to produce. Meeting needs has been difficult as a result.
B. Policy
Republic Act 7277, known as the Magna Carta for Disabled Persons, provides for the rehabilitation, self-development and self-reliance of people with disabilities and their integration into the mainstream of society. The Act provides for tax exemptions for donations to people with disabilities. Section 42, Item C, encourages the local manufacture of technical aids and appliances for disabled persons as a preferred area of investment.
The Philippines does not, at present, have national quality-control standards for assistive devices. The Philippine Association for Reintegration of the Disabled in Society (PARDS), an NGO, has been asked to investigate this question in coordination with Handicap International, the Department of Health, and the Philippine Academy of Rehabilitation Medicine. Research must be performed before standards can be laid down.
C. Production capacity
Each of the workshops established by Handicap International can manufacture an average of three BK and two AK prostheses a month, or 900 lower-limb prostheses annually. Other private agencies can each make six to seven prostheses per month or a total of up to 936 lower-limb prostheses annually. The manufacture of Jaipur-type BK prostheses is substantial, at 35 units per month or 420 annually. Local manufacture of upper-limb prostheses is less common, with only about five to eight limbs made per year. These are usually made by privately-owned workshops. Wheelchairs are produced locally at a rate of 30 chairs monthly or 360 a year.
Production is relatively limited for the following reasons:
- A limited number of workshops, in limited areas within the country;
- A small number of formally trained orthotists and prosthetists;
- A lack of trainers and training programmes for orthotists and programmes prosthetists;
- Non-availability of raw materials used for making devices, especially in the rural areas;
- High cost of technology and poor financial situation of users, making devices unaffordable;
- Conditions, such as medical complications, that make it difficult to apply a prosthesis or other device;
- A lack of awareness among community members, potential users and health professionals about the need for referrals and the availability of resources and devices.
D. Repair and maintenance
Repairs are supposed to be carried out by the workshops where devices are made. Often, however, they are undertaken by users themselves, family members, or local shoemakers.
E. Distribution
See diagram below.
F. Technology
The following equipment and machinery is used in the manufacture of prostheses and orthoses in the Philippines:
- socket-router plus tools
- suction pipe
- stand drill machine
- vacuum machine
- oven for thermoplastics
- zigzag sewing machine
- bandsaw
- steel shears
- grinder
- work bench
- bench-vice
- tools for gypsum room and mination
- IPOS deep drawing device
- magnetic lathe
- water balance
- screw drivers
- plaster cast cutter
- Sureform standard blade
- teflon tape
- plaster insulating cream
Locally available materials are used in the manufacture of many prostheses and orthoses. These include cowhide for the socket; wood and old rubber tyres for the foot; styropor, leatherette, and foam sheets for covering; and bicycle parts like iron, brake cables, wheel hubs, and nuts and bolts for the knee assembly. Lower-limb prostheses also use galvanized iron water pipes for the shaft; fibreglass, resin and hardener for the socket; and rubber and wood for the foot.
More expensive, high-technology components include modular prosthesis shafts, which are made of carbon-fiber composites, titanium, or aluminum alloy; hydraulic and pneumatic knee joints; ankle and foot components like the SACH, Carbon Copy or Seattle Foot; socket materials like laminated plastic chemicals, neoprene, polyethylene plastic and plastazote; cosmetic gloves and myoelectric components. Most of these components come from Otto-Bock and Gomed in Germany.
G. Personnel
Initially, in 1947, seven Filipino technicians from the Philippine Orthopedic Centre were commissioned to work with an American group of surgeons. Their apprenticeship consisted of assisting in the fitting of prefabricated prostheses, and in mechanical repairs and adjustments. They learned the mechanisms for knee joints and innovated means of adapting the socket to fit Filipino needs. Ten years later, two other Filipino technicians were sent to Australia under the Colombo Plan to train in making prostheses. The following year, those technicians, together with the Australian team, established a training programme for making orthoses and prostheses in the Philippine Orthopedic Center. Initially they were able to train 10 technicians who had come from different provinces of the Philippines.
Eleven technicians were initially trained by Handicap International, primarily through a hands-on and apprenticeship scheme. Recently, four additional technicians were trained by local technicians. At present, there is a plan to request UNIDO to help set up a training centre for technicians. It would be better still to have a training centre established by other countries in the ESCAP region.
Private technicians, being self-employed, earn more than those employed in workshops. The salaries of the latter are dependent on the ownership or status (government or NGO) of the workshops. In an NGO-affiliated workshop, the NGO is responsible for paying salaries, especially if the workshop is situated outside a hospital. In hospital-based workshops, the technicians receive their salaries, usually minimum wage, from the Government.
H. Institutional support
Sources of institutional support for the indigenous production and distribution of assistive devices are as follows.
(a) Governmental:
- (i) Department of Social Welfare and Development, especially, the Bureau of Disabled Persons Welfare;
- (ii) Department of Health, especially the Philippine Orthopedic Center;
- (iii) Department of National Defense, particularly the Armed Forces of the Philippines Medical Center;
- (iv) Department of Local Governments.
(b) Non-governmental:
- (i) Tahanang Walang Hagdanan;
- (ii) Our Lady of Victory;
- (iii) Mahaveer Foundation, Inc.;
- (iv) Simon of Cyrene;
- (v) Resources for the Blind, Inc.;
- (vi) VIDERE;
- (vii) PARDS;
- (viii) ABS-CBN.
(c) Foreign:
- (i) Handicap International;
- (ii) Goodwill Industries;
- (iii) AGAPE Sheltered Workshop, Japan;
- (iv) Christoffel-Blindenmission.
I. Technical cooperation
The Philippines will surely benefit from technical cooperation among developing countries. The Philippines has three technicians who can contribute substantially to other countries' technology. Definitely, it will be willing to send trainees to available training programmes, especially if these will be funded by an NGO. The Department of Health, Department of Social Services, UP-Philippine General Hospital and other NGOs can be the contacts for the Philippines in this exchange programme.
Comparative Costs of Various Appliances (US$)
| Device | Indigenous | Exoskeletal / Traditional | Modular / Imported |
| BK prosthesis | 40 - 100 | 320 - 400 | 1800 - 2000 |
| AK prosthesis | 160 - 200 | 800 - 1000 | 2600 - 2800 |
| Upper-limb prosthesis | N/A | 1000 - 1200 | > 14000 |
| Wheelchair | N/A | 96 - 100 | up to 360 |
| Cane | 4 - 6 | 20 - 30 | N/A |
| Crutch | 8 - 10 | 40 - 60 | N/A |
| Walker | 8 - 10 | 40 - 60 | N/A |
| Splint | 4 - 6/iny | N/A | N/A |
Go back to the Contents
ECONOMIC AND SOCIAL COMMISSION FOR ASIA AND THE PACIFIC
Production and distribution of assistive devices for people with disabilities: Part 2
- Chapter 9 to 12 -
ST/ESCAP/1774
UNITED NATIONS PUBLICATION
Sales No. E.98.II.F.7
Copyright © United Nations 1997
ISBN: 92-1-119775-9