The 3rd Asia-Pacific CBR Congress
Policy recommendations for the housing and environment modification services for persons with disabilities in Thailand
Sirinart Tongsiri MD. PhDi Chanutta Ployluemsaeng, PhDii Katanyu Hawsuthisimaiii
Introduction
Housing and environment modifications are essential to improve quality of life (QoL) of persons with disabilities (PWDs). The literature showed different supporting mechanisms of the modifications. In Australia, Housing Modification Funds are established in order to subsidize construction expenses to enhance functions of PWDs from unaffordable families to finance in whole or in part of the constructions1. In the US, mortgage loans are provided up to 25,000 USD for housing modifications in order to prevent the elderly or PWDs to be confined in hospitals2. The loans can be paid with no interest for 5 years.
In Thailand, according to the PWDs Empowerment Act (2007), registered PWDs are entitled to housing and environment modification services. The Provincial Social Development and Human Security Offices are responsible for the home modification services for PWDs. The access to the services is, however, hindered by many challenges, for example: the limitations of housing modification knowledge and systematic service provisions, inadequacy of accessibility features and family financial constraint. Community resource mobilization is one component under the Empowerment Sector of the WHO Community-based Rehabilitation (CBR) Matrix. For those unable to afford the housing modifications, community resource could be used to subsidize for the services.
Our research aimed to develop policy recommendations to improve the service accessibility and to suggest how the resources should be mobilized in Thailand.
Methods
The group of persons with mobility difficulties and the elderly according to the proposed criteria was recruited by physical therapists or primary care nurses from 4 provinces: Khonkaen, Mahasarakham, Kalasin and Roi-Et. Each participant was evaluated using the International Classification of Functioning, Disability and Health (ICF)-based questionnaire, EQ-5D-3L, Berg Balance Scale Test and the home and environment assessment form. The designated criteria were difficulties in walking (ICF codes d450 with qualifiers 2, 3 and 4), ownership of the house and willing to accept the services. Home environments and functions of the participants were also recorded in photographs and short vdo clips.
Capacity building sessions for architects, engineers, local builders, nurses, social-workers were conducted to give more insights of appropriate housing and environment for PWDs. Then the architect who was part of our research team completed the housing measurement followed by producing house plans where changes were clearly indicated. The design of appropriate home modifications was based on the universal design concept according to the functions of individual PWDs. Constructions began after the modification plans were approved by all including PWDs themselves. The researchers consequently visited construction sites and checked whether the construction protocol and plans were met. Changes in the modifications could be initiated when the researchers considered the achievement of higher benefits in improving Qol of PWDs. Function of PWDs before and after modifications were evaluated immediately after complete the construction process and at 3, 6 and 9 months respectively, using the questionnaire based on the International Classification of Functioning, Disability and Health (ICF). Available financial resources were explored by researchers.
Costs of all construction processes were recorded. The data of costs and the functions changes will be proposed to policy makers to develop national policy and allocate resources to support the housing modification process.
Results
The data collection had been conducted during January to April 2014. The total of 62 participants were selected and examined at their home settings. The mean age of the participants was 57.3+17.2 years and approximately half of the participation were male (52%). Almost all of them (98%) suffered from some degree of walking difficulties (d450.1-d450.4). The most common activity performed with difficulties was getting up from floor and getting up from chair or bed. Five persons died before the construction started. Two persons later denied the modifications and six houses awaited for the funding, therefore, not to be included in the report. In total, forty-nine houses were successfully modified. The majority functions improved after the modifications were walking, getting up from chair/bed, climbing stairs, moving outside home, getting up from floor and moving inside home.
Resources for the services were drawn from the provincial rehabilitation funds, sub-district administrative organizations as well as the contributions from PWD families. Construction workers were mainly volunteers from community for example, Buddhist monks, villagers, solders from the local army, villagers and family members. In the areas where volunteers were unavailable, professional builders were hired.
The modification types were classified into 4 groups according to costs of construction and the modification features. Group 1 included those with minimal degree of modification such as installing handrails or building extra-wide doors. Average cost of Group 1 was 20,922.05 baht (approximately 620 USD). Group 2 was those with the changing some part of the houses, for example, relocated toilet to be near living area. Group 2 average cost was 41,519.30 baht (approx. 1,235 USD). Group 3 consisted of the houses unable to be modified and newer houses were built. The average cost of this group was 63,918.15 baht (approx. 1,890 USD). Group 4 was those which the modification priority was assigned to the security of the house rather than to improve PWDs’ function, such as to build new roof or to fill the land for flood prevention. The average cost of Group 2 was 23,000 baht (approx. 700 USD). Construction durations were 2-15 days for Group1, 3-20 days for Group 2 and 11-30 days for Group 3. Qol measured by EQ-5D-5L were increased 0.158 in Group 1, 0.164 in Group 2, 0.348 in Group 3 and 0.203 in Group 4.
Discussion
The housing and environment modifications services can be made available for those PWDs with difficulties accessing the services due to financial constraint and the limitation of service availability in community. Not only financial support from community resources but also knowledge of the modifications of part of the house or building a new house should be increased. The modifications should mainly be provided for enhance PWD functions therefore the housing modifications may not be in line with standard housing. Multidisciplinary team should involve those from health care sectors and from non-health care sectors, for example, architects, social workers and local administrative organizations. Additional changes were not uncommon after completing the modifications due to PWD requirements.
We recommend that to provide the service, the following procedure should be considered: stakeholder linkage, resource integration and allocation, decision making based on functioning data and capacity building. Knowledge management should be conducted to add more knowledge and understandings. Policy makers may earmark the budget for PWDs housing and environment modifications using the costs provided by this study.
Summary
Housing and environment modifications can improve PWDs functions as well as qol. For those with difficulties to access the modification services, resources should be systematically cooperated from various community organizations.
Reference
1. The Victorian Department of Human Services (2009). Disability Services-Aged Care Assessment Protocol. Melbourne, Victoria. Downloaded from http://www.dhs.vic.gov.au/disability
2. Illinois Housing Development Authority. Single-Family Owner-Occupied Rehabilitation (SFOOR) Program. Downloaded from http://www.ihda.org/homeowner/grantHomeowner.htm#SFOOR. Accessed date 2 February 2014.
i Faculty of Medicine, Mahasarakham University. E-mail address: stongsiri@yahoo.co.uk
ii Faculty of Pharmacy, Mahasarakham University
iii Faculty of Architecture, Urban Design and Creative Arts, Mahasarakham University
Slide 1 (Slide 1 text)
(Slide 1 text)
Slide 2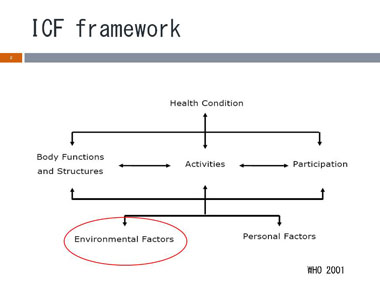 (Slide 2 text)
(Slide 2 text)
Slide 3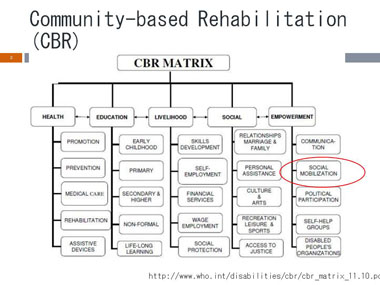 (Slide 3 text)
(Slide 3 text)
Slide 4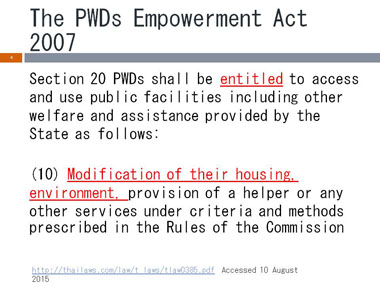 (Slide 4 text)
(Slide 4 text)
Slide 5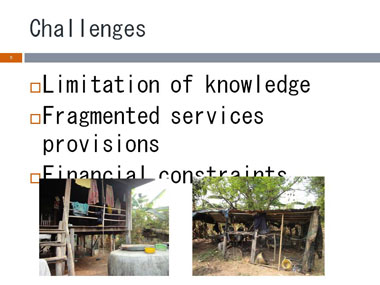 (Slide 5 text)
(Slide 5 text)
Slide 6 (Slide 6 text)
(Slide 6 text)
Slide 7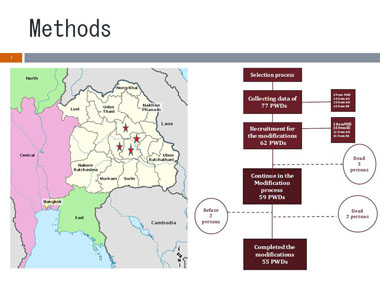 (Slide 7 text)
(Slide 7 text)
Slide 8 (Slide 8 text)
(Slide 8 text)
Slide 9 (Slide 9 text)
(Slide 9 text)
Slide 10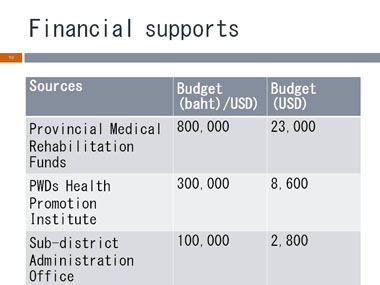 (Slide 10 text)
(Slide 10 text)
Slide 11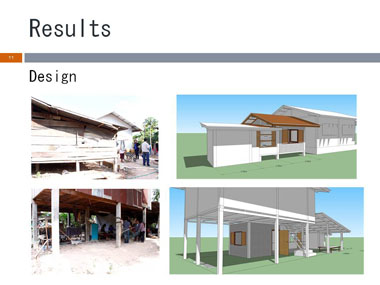 (Slide 11 text)
(Slide 11 text)
Slide 12 (Slide 12 text)
(Slide 12 text)
Slide 13 (Slide 13 text)
(Slide 13 text)
Slide 14 (Slide 14 text)
(Slide 14 text)
Slide 15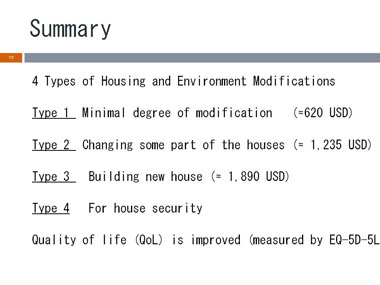 (Slide 15 text)
(Slide 15 text)
Slide 16 (Slide 16 text)
(Slide 16 text)
Slide 17 (Slide 17 text)
(Slide 17 text)
Slide 18 (Slide 18 text)
(Slide 18 text)