The 3rd Asia-Pacific CBR Congress
Information on CBID practices to be organised according to the following sections
Community Based Inclusive Development: Our way of approaching it!
- Community: Group of People living in one particular geographical area; in case of KFN: Village Development Committee
- Inclusive: To accommodate all types of people living in the same geographical area, all people should be freely and openly accommodated without restrictions or limitations.
- Development: Progressive changes (+) in the lives of people; contextual
Community Based Inclusive Development (CBID) means meaningful participation in every development activities of all types of people of the community living in same area. CBID is an approach of social development which not only ensures the sustainability of any development initiative but also respects the self-esteem of the people and increases social cohesion among the community members.
Likewise, inclusive development putting means that partnerships and alliances are necessary between different stakeholders, especially between Community Based Rehabilitation (CBR), Disabled People’s Organization (DPOs), Families of Persons with Disabilities and Government actors (Thomas et al, 2010).
Section 1
Background: Country, whether CRPD is signed and ratified, any national laws and policies, percentage of population of persons with disabilities
Situation of Persons with Disabilities in Nepal’s Community Based Inclusive Development (fact and figure- policies, provisions, guidelines)
The National Census of 2011 reports that Persons with Disabilities in Nepal constitutes 1.94 percent of the total population. In the meantime, World Health Organization estimates that 15 percent of the total population is what Persons with Disabilities contribute to the total count.
In Nepal, most of the families with adults /children with disabilities are in the category of Below Poverty Line (BPL) which makes them marginalized of the marginalized. There are no organization and structure available in the communities which are working and specialized in CBR. Reach of CBR programs in rural communities is yet a challenge in Nepal. In the health facilities all medical problems are viewed as curative case and are not considered, anyway, from disability prevention and rehabilitation perspective. Education and livelihood services are still far from the reach of persons with disabilities and their families.
However, there are many laws that have been developed in Nepal for the welfare of Persons with Disabilities. After Nepal ratified United Nations Convention on Rights of Persons with Disabilities (UNCRPD) in 2009, the laws of Nepal are in the process of revision to align them with the provisions made in UNCRPD.
Act, Policies and Guidelines in Nepal
- UNCRPD ratified by Nepal in 2009; Its optional protocol on..???
- Disability Protection and Welfare Act, 1982 (2039 B.S.), which is in the process of amendment.
- The special education act also is being revised.
- Most importantly the upcoming constitution of Nepal is going to incorporate the disability issues in Fundamental rights and political rights with positive reservation in many clauses.
- National Policy and Plan of Action on Disability, 2006- in the process of revision
- Community Based Rehabilitation Guideline- in the process of revision
- Accessibility Guideline, 2013 approved by Cabinet and in the process of implementation
- Personal Assistant Guideline development ongoing.
1.1 Project area: population covered, number of persons with disabilities in the area, general situation of persons with disabilities, needs and challenges
The general situation of the Persons with the disabilities in the project area is same as elsewhere, not recognized, not accepted and deprived. The needs are huge and wide ranges and the challenges are to address the needs changing the mindset and establish regular supply and service centers.
Major Projects of Karuna Foundation (Phase- 1, 2008-2013)
| S.No. | Projects | Project Sites | Total Beneficiaries | Children with Disabilities | Total population p ersons with disabilities (census 2011) |
|---|---|---|---|---|---|
| 1 | Rasuwa | Inspire2Care (4 VDCs) | 19,600 | 144 | 380 |
| Share&Care (Syafru) | |||||
| 2 | Sunsari | Inspire2Care (3 VDCs) | 103,460 | 464 | 1863 |
| Share&Care (5 VDCs) | |||||
| 3 | Kavre | Share&Care (3 VDCs) | 11,800 | 145 | 229 |
| 4 | Policy, Awareness, Advocacy & Networking | At central level and project district level | |||
| Total | 134,860 | 753 | 2472 |
1.2 When did this project start, how did it start, what was the motivation to start, what are the main objectives? Management and organization – who manages,?
This project was started in 2008. An entrepreneur from the Netherlands named Mr. Rene Aan de Stegge has a daughter born with spinabifida. She is 18 years old now and in well health and physical condition. Rene and his wife, Briggitte have demonstrated an example by giving their every support and care to this girl child, otherwise it would not be possible to see her as a perfect young girl today. She gave huge confidence and willingness to the couple to contribute towards prevention of childhood disabilities and disabilities in general.
Nepal was selected as a first country to implement the project. We developed two specific Objectives: Prevention of Childhood Disabilities (birth defects and early identification) and Community Based Rehabilitation for Children/Adults With Disabilities.
With the success of the first phase, we have decided to expand the project covering a whole district (covering 300.000 population including people with disabilities) aiming to demonstrate a successful district wise model. This project will be implemented in phases; in three years and it will cover the whole district.
Section 2
2. What are the main activities according to the CBR Matrix, how do they follow the twin track approach in their work?
We precisely follow the five by five boxes of CBR Matrix as per the need and service/resource availability. We are also working with the ministry to revise and introduce the Community based Rehabilitation guidelines.
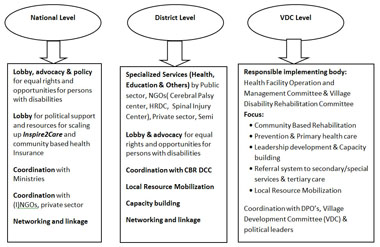
The activities on different levels:
National Level
On a national level we will work mainly on:
- Lobby and Advocacy for equal rights and opportunities for people with a disability: Lobbying with policy influencers, CRPD implementation and collaboration in the scaling up and after.
- Changing societies and their attitudes: creating an enabling environment for people with a disability
District and Community level
On the district and the community level we will work on the following programme components:
- Changing societies and their attitudes: creating an enabling environment for people with a disability
- Capacity Building of the different stakeholders and community mobilisation: Capacity building with a focus on institutional and human resource strengthening. Existing partners such as the CP Centre will be used to train social health workers and community based rehabilitation facilitators. Furthermore a referral network between primary and secondary/tertiary levels will be established.
Primary level
Program wise- identification, assessment, needful intervention in all areas coordination, lobbying at local level, c etc. existing structures within the system will be enhanced so that they could realize their responsibilities and act accordingly. HFOMC/VRC will act as primary care providers together with families and make needful referrals in case of secondary/specialized services ranging from health and education; vocational training and livelihood.
Financial sustainability of the level will be achieved after 5 years. In Karuna Foundation Nepal's first phase project VDCs local resources have been mobilised optimally together with local human resource mobilizations which has lead the projects toward financial sustainability. This will be replicated with improved knowledge in this expansion phase.
Secondary and tertiary level
Secondary level services are medical, rehabilitative and non- medical services and those services which can't be provided at the community level either for not having the services or skills. These services could be governmental and non -governmental organizations with special expertise.
- A separate agreement will be made with these kinds of organizations to provide the services to the needy persons. Required support will be provided to these organizations to strengthen the organizational capacity for high level and effective services. The specialised services also include tertiary services.
Community Based Rehabilitation
The programme focuses to the 5 different domains of Community Based Rehabilitation:
- Health: Under the component health the Joint Venture will work on health promotion and prevention of disabilities via primary level stakeholders. These stakeholders will also be responsible for basic medical care, rehabilitation and provision of assistive devices. For more complex cases a referral system to secondary and tertiary level will be established.
- Education: Early childhood and informal education will be established with the communities. Promotion and creating awareness of the importance of education is key in early stages. Community workers will discuss the enrolment of persons with a disability in mainstream primary, secondary and higher education where possible. The Joint Venture will advocate to inclusive education in Nepal.
- Livelihood: The Joint Venture will have a strong focus on livelihood and income generating activities. In order to achieve economical sustainable activities the average income of the target group will have to be increased. Increased savings and health insurance will facilitate independent access to services in the future.
- Social: An important component in the programme of this Joint Venture is the social aspect. Having equal rights and opportunities for marriage, participate in sports programmes, cultural activities and most important have equal access to justice is utterly important for long term success.
- Empowerment: DPO and SHG formation are an important component in the programme. The programme targets to support people with a disability in raising their own voice and become self-advocates for their own rights.
Prevention & Primary Health Care
The program will focus on Prevention of childhood disability and early detection and intervention. It will be achieved through strengthening primary care mainly on maternal child health issues. It is basically safe pregnancy-safe delivery -safe infancy.
Section 3
3. Who are the key stakeholders? What is the role of persons with disabilities in the project? What is the role of Government? Any partnership between government and NGOs/DPOs?
The major key stakeholders of the project are the District Health Office, District Development Committee, Women and Child Development Office and their VDC level units and VDC level self-help group and DPO. The role of the persons with disabilities is crucial as they decide what short of program has to be designed and implemented. Furthermore we use spice indicators to measure the success developed/defined by the right holders themselves.
Major issues and structures
Section 4
4.1 What was the impact of the project at individual and community level? How was this impact measured? What is the basis for claiming impact?
7. Major Achievements
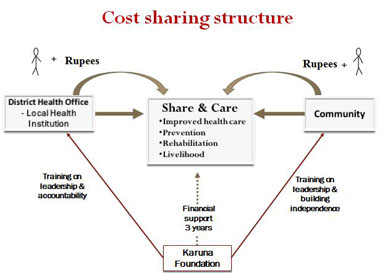
7.1 Share and Care
- Nearly 64,753 person years (21.3%) out of 303,326 person years were financially protected through health insurance scheme
- Nearly 242,661 person years (80% of total person years) utilized the improved health care services. Out of this 58,278 (24%) person years were the members and 184,383 (76%) person years were non-members.
- total of 1818 members out of 64,753 members in 6 years (2.6%) got financial protection for hospital referral expenses.
- total of 497 families (4.5 % of total households in project VDCs) below poverty line received loans which they utilized for income generation.
- We tried to include as many households as possible into the system (25% of the total households and 40% of households within reach of Health Facilities are now members)
- We covered an entire region or cluster of VDCs so that adjacent VDCs share ideas and learn from each other, and the program operation also becomes easier.
- Now, the local health systems in the program VDCs accept it as their regular business.
7.2 Inspire2Care/Disability Prevention and Rehabilitation
- Birthing centers have been supported in 7 sites
- Strengthening of Primary Health Care /Out Reach Clinic has been done in all program VDCs
- Day celebrations, street drama presentations and orientation on reproductive health issues were conducted in project VDCs
- A total of 747 children with disabilities have been identified. Out of this, 108 children (14%) with disabilities have been successfully rehabilitated in their communities through the CBR approach.
- Our experiences show that the CBR program could be organized effectively and at a lower cost if a wide range of stakeholders are involved.
- CBR approach can create unbelievable impact in the life of children with disabilities and their families.
- Community people are focusing to include person with disability and their families in every community development activities and also starting to create surrounding environment inclusive and friendly.
1. CBID impact in the lives of Persons with Disabilities
- Children with disability have been getting equal access to right to education, health care, social participation. They are able to go to school, participating in social events after the rehabilitation intervention.
- Recognition and acceptance from family and community people has been increased. Children have been participating in indoor and outdoor activities without any hesitation and restriction.
- Economic status of their family has been increasing after involving in livelihood program.
- Empowerment of community people and parents of children with disability
- Community people focusing in inclusion of person with disability and their families in development process and also creating inclusive and disability friendly environment in community.
- All children and adults of the project areas are identified and have individual profile.
- Access to Government provisions/ schemes i.e. cash allowances, scholarship has increased
2. CBID impact on Lives of Persons with Disabilities in the community
- Implementation, leadership and ownership on program by local community
- Local resource mobilization and proper utilization
- Recognition and acceptance to person with disability in their community
- Increasing participation of person with disability in social development
- Empowerment of community people, leaders
- Increasing awareness/sensitization level of community about inclusive development
4.2 What are the key lessons learned? What can others learn from this project if they want to start work in this area?
The major lessons learned are:
- Disability could be prevented, and we have to put efforts on both prevention (Birth defects and secondary prevention) and rehabilitation in an inclusive manner
- Awareness rising on disability to politicians, bureaucracy, media people, teachers and the health workers is the key.
- Once people are aware they are positive and committed to support
- Disability related programs are not as expensive as considered if started from the very beginning and in an organized way.
- The population is scattered , the nature is diverse and most importantly the data is not available
- Dependent thinking of Persons with Disabilities and their families
Replicability/ adoptability
- The work could be easily started in any part of the globe if there are some committed but out of box thinking people. Disability is developmental agenda thus is a political agenda. Until and unless the politics do not recognize it and accept it can't be well organized.
- WE need to start from the bottom, identifying the disabled population, assessing their situation and most importantly involving family as a key player so that the ripple gets larger.
- Technology has greater role to play to improve the quality of life of persons with disabilities and rich and developed countries has to play a positive and humanitarian role to transform the technologies and make it assessable to the poor countries.
- Disability cannot be dealt in isolation. Everybody has to be involved and must be sensitive.
Section 5
5. What are the sources of financial support?
From Karuna Foundation Holland and other individual and foundations.
Community, Local and Central government
Section 6 6.1 What are the future plans?
Expansion of the project
The project is ready to start the first batch in June 2014 in 15 villages in Jhapa, Ilam and Rasuwa (Optional in case of Rasuwa). The program will be further expanded to other villages in these 2 districts upon reaching the set milestones at the end of 2015 (refer below mentioned milestones). The longer term project plan is to cover whole 48 VDCs and 1 Municipality of Ilam and remaining 13 VDCs of Rasuwa (5 VDCs already covered).
The detailed plan including budget, context analysis and structure has been developed and Karuna Foundation Nepal is ready for implementation. Following are the project beneficiaries or target group for three districts in five years:
| 2014-2018 | First phase 2014 | Second Phase 2015/16 | Third phase 2017 | |||
|---|---|---|---|---|---|---|
| Rasuwa | Ilam | Jhapa | 3 VDCs in average, estimated | |||
| Total population | 43,300 | 290,254 | 812,650 | 41,950 | ||
| Total HHs | 9778 | 64502 | 184552 | |||
| Women of childbearing age* | 10,514 | 83,298 | 233,217 | 29,177 | ||
| Children under 5 years* | 3,755 | 20,494 | 57,379 | 2'936 | ||
| Children with a disability** | 260 | 1,762 | 4,933 | 251 | ||
| Persons with a disability* | 1,016 | 7,636 | 21,379 | 570 | ||
| target population | 15,545 | 113,190 | 316,908 | 32,934 | ||
6.2 How will the project sustain the activities in CBID?
Sustainability
For KFN, sustainability has three major domains which are:
- Financial Sustainability is related to all about financial resource mobilization and its proper management based on the cost sharing principles.
- Structural Sustainability deals the management issues of the program including mobilization of all the stakeholders, networks, lobbying and creating positive environment. Timely and accurate recording and reporting in a transparent manner.
- Quality Sustainability covers the areas of providing best possible quality services through improvement/strengthening of service providers, needful linkages and/or referrals to secondary and tertiary care and assistive/supportive devices.
After 5 years
Impact
- 10-20% decrease in birth defects
- 30-40% decrease in disabilities among children because of diseases, accidents, burns, malnutrition
- 75% of the children with a disability experiences a significant improvement in the quality of life because of progress and change in health, education, independence, empowerment, social life, income.
- 25% of the adults with a disability experiences a significant improvement in the quality of life because of progress and change in health, education, independence, empowerment, social life, income.
- An evidence based sustainable CBR and prevention model ready to be replicated.
In society the attitude and perception on disability has changed and children and adults with a disability are included more in the community and participate in events, meetings etc.
System impact: to be formulated!
Results
CBR, integrated care and inclusion
- 2000 children with a disability have improvement in their health and mobility because of treatment, physiotherapy, operations, assistive devices, vaccinations, improved nutrition etc.
- 2000 children with a disability and their families have access to health care, education, vocational training, loans, income.
- 2000 adults with a disability, including due to leprosy have experienced improvement in their situation and have access to basic services
- 1000 adults with a disability have increased their income through a livelihood program or a self- help group.
Prevention of disabilities
- Basic services for care during pregnancy, delivery and infancy have improved in quality and accessibility. The health management information system has been strengthened.
- 60% of the pregnant women have 4 full antenatal check-ups, including iron/folic acid supplementation and vaccinations.
- 60% of the deliveries take place in a health institution.
- 95% of the children under-5 is fully immunized against diseases such as polio, measles and tetanus.
Local ownership and sustainability
50 villages (80%) continue to carry out Inspire2Care after 3 years successfully with good leadership, governance and financial sustainability.
- Change of society’s perception of ultra -poor and people with a disability, because of its focus on the strength and dignity of people and by inspiring them to reach their full potential.
- Empowerment of people through a truly bottom-up approach with decentralized decision making power at local level. Participation of people and their representatives in need identification, planning, implementation and monitoring is the key to success. Financial participation encourages people to claim their rights.
- Strong local leadership and good governance by implementing a clear-cut structure and building capacity of local leaders, health providers and civil servants Share & Care encourages people to become responsible and accountable while using local resources and creating sustainable solutions
- Inclusion of marginalized groups (below poverty-line families, (ethnic) minorities, women, children, disabled and elderly). Commitment and sensitiveness towards the health rights of marginalized people with interventions to make sure that they participate. It advocates against subsidy and looks for dignified ways of involvement i.e. livelihood options, money for work.
Slide 1 (Slide 1 text)
(Slide 1 text)
Slide 2 (Slide 2 text)
(Slide 2 text)
Slide 3 (Slide 3 text)
(Slide 3 text)
Slide 4 (Slide 4 text)
(Slide 4 text)
Slide 5 (Slide 5 text)
(Slide 5 text)
Slide 6 (Slide 6 text)
(Slide 6 text)
Slide 7 (Slide 7 text)
(Slide 7 text)
Slide 8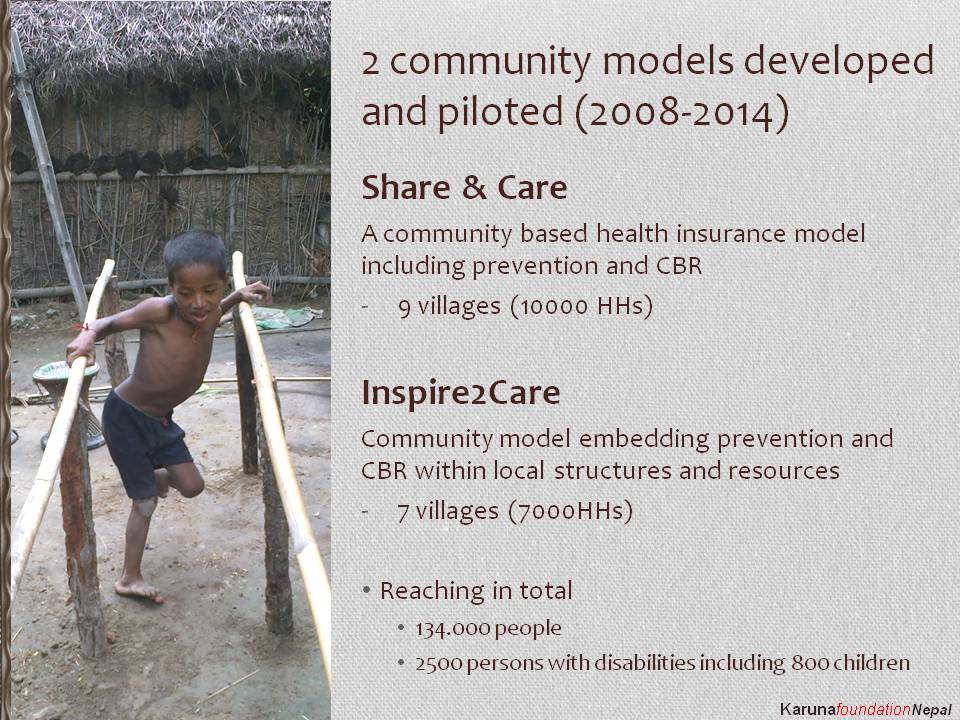 (Slide 8 text)
(Slide 8 text)
Slide 9 (Slide 9 text)
(Slide 9 text)
Slide 10 (Slide 10 text)
(Slide 10 text)
Slide 11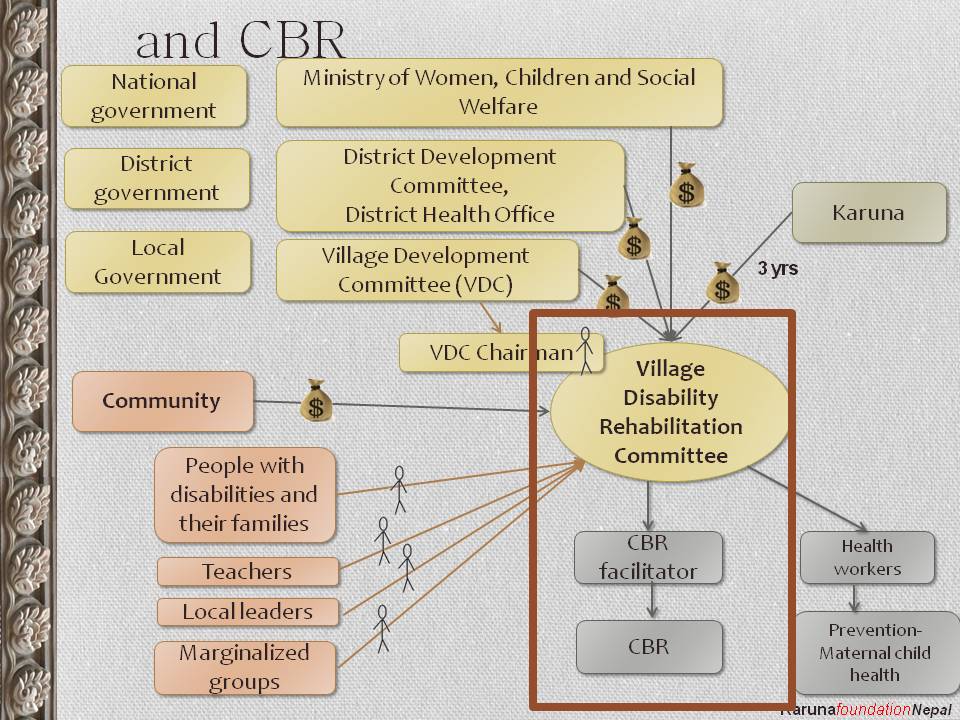 (Slide 11 text)
(Slide 11 text)
Slide 12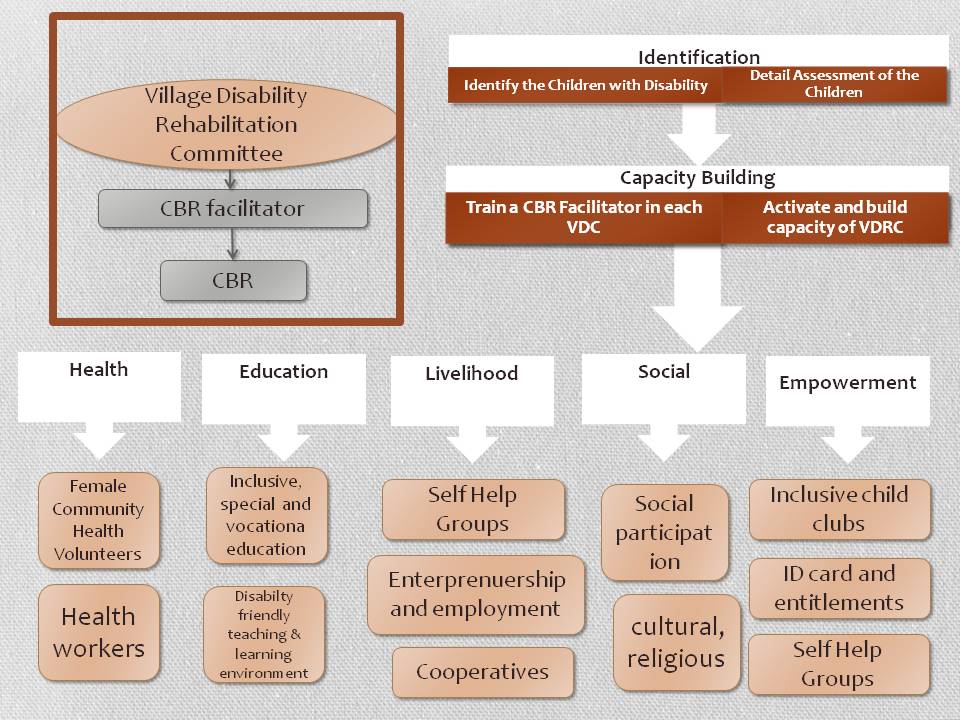 (Slide 12 text)
(Slide 12 text)
Slide 13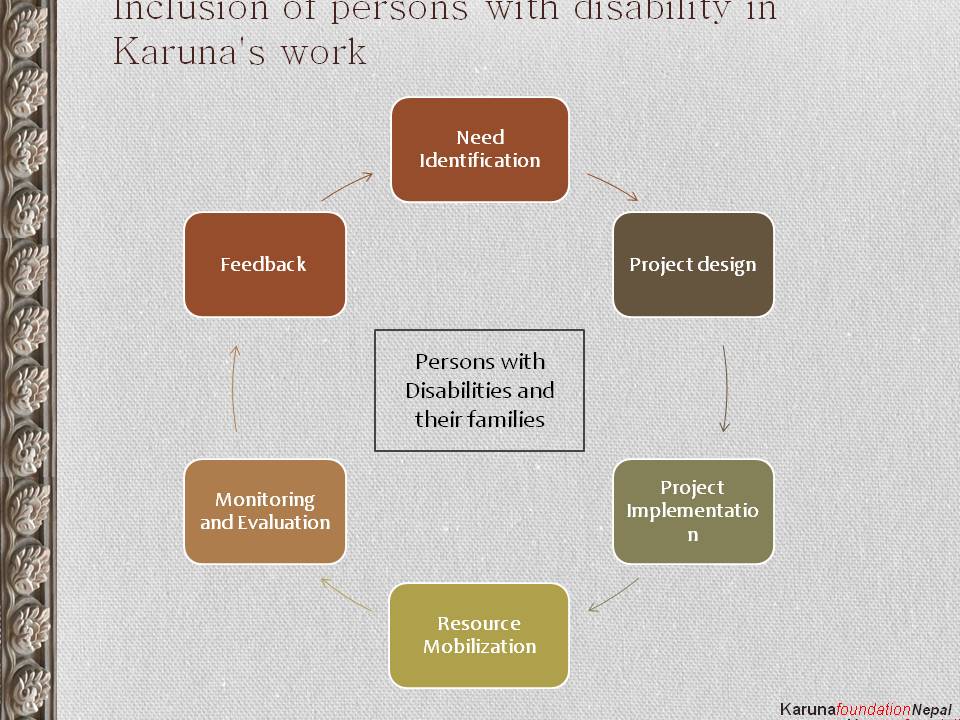 (Slide 13 text)
(Slide 13 text)
Slide 14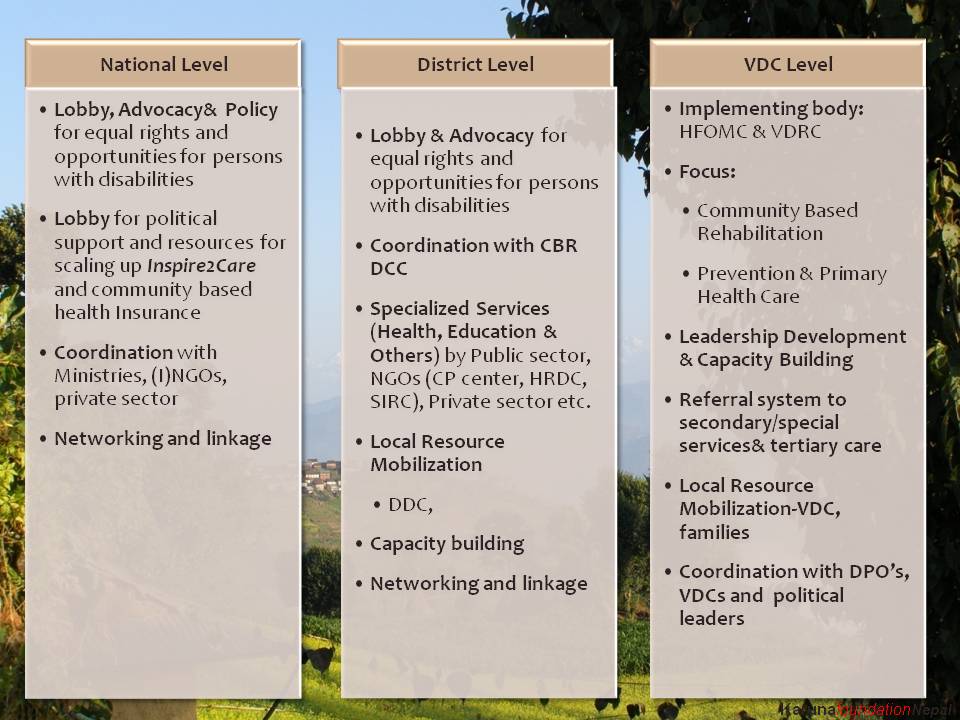 (Slide 14 text)
(Slide 14 text)
Slide 15 (Slide 15 text)
(Slide 15 text)
Slide 16 (Slide 16 text)
(Slide 16 text)
Slide 17 (Slide 17 text)
(Slide 17 text)
Slide 18 (Slide 18 text)
(Slide 18 text)
Slide 19 (Slide 19 text)
(Slide 19 text)
Slide 20 (Slide 20 text)
(Slide 20 text)
Slide 21 (Slide 21 text)
(Slide 21 text)
Slide 22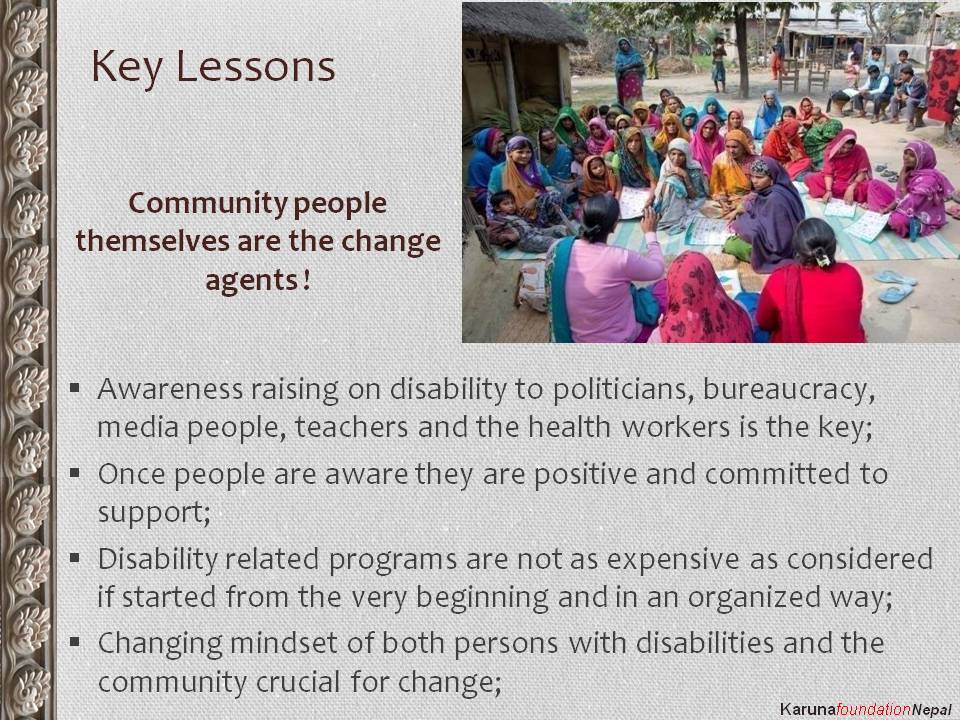 (Slide 22 text)
(Slide 22 text)
Slide 23 (Slide 23 text)
(Slide 23 text)
Slide 24 (Slide 24 text)
(Slide 24 text)
Slide 25 (Slide 25 text)
(Slide 25 text)
Slide 26 (Slide 26 text)
(Slide 26 text)
Slide 27 (Slide 27 text)
(Slide 27 text)