PREVENTING THE RISK OF FALLING IN ELDERLY PATIENTS
Pietro G. Morasso
1University of Genova - DIST,Via Opera Pia 13, I-16145, Genova, Italy
tel: + 39 10 3532749, fax: + 39 10 3532154, email: morasso@dist.unige.it
Center of Bioengineering, Hospital La Colletta, Via Giappone 3, I-16011 Arenzano, Italy
tel: +39 10 9134805; fax: +39 10 9134122; email: morasso@dist.unige.it
Luigi Baratto
Center of Bioengineering, Hospital La Colletta, Via Giappone 3, I-16011 Arenzano, Italy
tel: +39 10 9134805; fax: +39 10 9134122; email: colletta@csita.unige.it
Roberto Capra
2Center of Bioengineering, Hospital La Colletta, Via Giappone 3, I-16011 Arenzano, Italy
tel: +39 10 9134805; fax: +39 10 9134122; email: colletta@csita.unige.it
Gino Spada
2Center of Bioengineering, Hospital La Colletta,Via Giappone 3, I-16011 Arenzano, Italy
tel: +39 10 9134805; fax: +39 10 9134122; email: colletta@csita.unige.it
1. Summary
An open posturographic system is described which is aimed at preventing the risk of falling in elderly patients and in general is intended as a tool for the quantitative evaluation of balance disorders. The system is characterised by simplicity and low-cost and particular emphasis is put on the integration between research and the clinical constraints typical of a rehabilitation hospital; a systematic clinical validation is underway in different rehabilitation sites, which feeds back immediately on the research activity.
| Top |
2. Introduction
In a project supported by the Higher Institute of Health in Rome a clinical protocol for the evaluation of balance disorders has been designed which complements and enhances standard clinical tests with techniques of movement analysis for preventing the risk of falling in elderly patients. The protocol is meant as a screening and monitoring tool to be applied to a large but focused population of healthy elderly, in order to increase their chances of maintaining a substantial degree of autonomy in their normal activity. It is known indeed that autonomy is dramatically impaired not only by the consequences of actual falls but by the fear of falling as well. Simple measurements such as the average walking speed (Bronstein et al. 1996) have been demonstrated to discriminate in a reliable manner the populations of fallers and non-fallers, but are not informative enough for being directly useful at the clinical level, i.e. in relation with the individual patient. On the other hand, the complexity of the postural control system is still an open research issue (Perrin and Lestienne 1994) and it is not possible to design a "complete" experimental setup, capable to identify all the parameters of the different control subsystems and differentiate among specific pathological conditions. Therefore, the design of the experimental setup was guided by a number of different considerations: (i) technical simplicity, in order to achieve a low-cost of the equipment (ii) operational simplicity, characterised by organisational low-cost in terms of the amount of preparation/calibration effort and duration of the examination, (iii) compatibility with the routine clinical conditions in a rehabilitation environment (iv) clinical significance and complementarity with non-instrumental observations, (v) modularity of the experimental setup, which should be easily adapted to a range of needs and a hierarchy of requirements at the different levels of the health care delivery system (from the ambulatory level to the level of regional or national rehabilitation centres).
These requirements guided the selection of the type of equipment and the experimental paradigms and the integration in an open measurement system. The main decision was to focus the attention on posture rather than gait, taking inspiration from and aiming at the integration with the test developed by M.E. Tinetti (1986). As a consequence, we decided to avoid the use of the expensive equipment typically used in gait analysis, which is based on optoelectronic systems, 3-D force platforms and multi-channel electro-myography, ending up with a simple but flexible open posturographic system, which is described in the next section. From the clinical point of view, it was decided that the measurement protocols should be restricted to a population of elderly subjects (aged over 65) who are characterised by the absence of severe pathological conditions, have a good degree of autonomy but exhibit some problem of balance. In particular, we defined a set of inclusion criteria, for the pre-selection of the subjects to be given the posturographic tests, which were based on standard clinical scales:
(1) Co-morbility index (Parmelee 1995) CIRS; it is based on 14 pathologic categories, with a 5 grade scale; the criterion of inclusion is that in no category the rating scale must exceed 3;
(2) IADL index (Katz et al. 1970); it is based on 6 categories of activities of daily living, from the most complex (AD1=bathing) to the simplest (AD6=feeding) rated according to the degree of independence; the criterion is total independence in all categories except AD1;
(3) Tinetti Index (Tinetti 1986) which grades the performance in a number of gestures which are crucial for a stable balance; the criterion is that the total score must be close to the maximum: ³ 14/16.

Fig. 1 Open posturographic system.
The system (Fig. 1) consists of a simple 2-D force platform , integrated with a piezoresistive sensor (Fig. 2), a configurable set of accelerometric/inclinometric sensors, and an environment stimulation system which can provide simple visual, acoustic and mechanic stimuli. The measured gestures, in agreement with the Tinetti's index, are essentially transfers of weight load between sitting and standing postures and different gestures in the standing posture. The developed software allows to choose between two types of protocols: a basic protocol, to be administered to all the elderly subjects identified according to the inclusion criteria and a range of second-level, to be tailored for the specific problems of selected patients and aimed at monitoring the time evolution of the functional performances.
| Top |
3. The open posturographic system
The basic protocol only uses the information of the time course of the centre of pressure on the support platform (Baratto et al. 1997), with the freedom for the patients to choose a comfortable (Romberg) position of their feet, and consists of a fixed set of 7 gestures:
1) standing with open or
2) closed eye;
3) and 4) sensitised standing with open eyes (one foot in front of the other);
5) standing up and sitting down;
6) reacting to a sudden pushing force in the chest ;
7) turning 360° on the place.
Classical posturographic parameters are evaluated, such as the sway-path and sway-area. Innovative techniques are also being developed (Baratto et al. 1996) which attempt to isolate in the evolution of the centre of pressure episodes of relative stabilisation/destabilisation which seem to better discriminate between normal and pathological conditions than the purely numeric comparison of the classic posturographic parameters. The session has been automated in such a way to last 10-15 minutes and to require the intervention of only one person. As regards the sitting/standing gestures, it was decided after the initial experimentation that the instrumentation of the seat was not worth the additional cost. The pushing gesture turned out to be much more informative (and more "ecological" for the elderly patients than the sudden displacements/rotations of the support base which are typically used in some expensive systems) and a prototype of a simple strain-gauged instrumented hand-held pushing device is in the course of having a clinical validation, together with a trunk-attached 2 degrees-of-freedom inclinometer which can help to estimate the relative contribution of the hip strategy vs. the ankle strategy in the stabilisation of the standing posture.
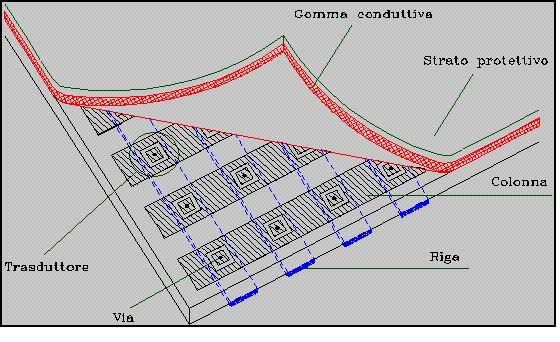
Fig. 2. Piezo-resistive sensor
In the second level set of protocols, the experimenter can personalise the experimental parameters and choose from a menu of possible experimental conditions which also allow a number of biofeedback/rehabilitation paradigms. In the simplest case the user is given a visual feedback of the position of its feet superimposed with the centre of pressure. This can be coupled with visual or acoustic stimuli which provide targets for the centre of pressure, changed in a random or periodic, rhythmic fashion. Acoustic rhythmic paradigms, which mimic dancing gestures, are also in the course of clinical evaluation with promising results, which confirm the background knowledge that rhythm is a great motor organiser; the experimental setup allows to manipulate the rhythmic patterns and, at the same time, evaluate the functional improvements form the posturographic point of view.
| Top |
4. The clinical experience
The basic system is meant to be disseminated at the ambulatorial level as a basic tool for screening the patients at risk. The pilot experimentation is currently being carried out in three centres: (i) the posturographic ambulatory at the Hospital in Arenzano (Genova), (ii) the AISM centre in Imperia, and (iii) the Golgi Geriatric Institute in Abbiategrasso (Milano). More than 200 cases have already been collected with the basic protocol and are evaluated.
In Arenzano two additional clinical investigations are carried out in which the posturographic analysis is coupled with other important clinical observations. The larger experiment is a screening campaign carried out by the Rheumatological division of the hospital which is related to osteoporosis and collects for the same patients data about bone densitometry and postural stability. A significant correlation has already been found at the population level: the next step is to investigate finer discriminations which can be applied at the individual case. In a smaller clinical study, in co-operation with the Neurologic Department of the University, Parkinsonian patients are analysed, looking for analogies and significant correlations between the spatiotemporal patterns of posturographic and handwriting data.
| Top |
5. Conclusion
The clinical validity of the analysis of posture, which in recent years has been overshadowed by the new techniques in gait analysis, is worth a renewed effort, both at the theoretical and technological levels. From the point of view of motor control theory we intend to explore the theme of self-organisation (Morasso and Sanguineti 1997), which brings together neural plasticity and the mechanical properties of the peripheral apparatus. This is particularly true in the case of balance which is typically a multi-sensory, multi-factorial system. From the experimental point of view, we think that the empiric knowledge coming from the posturographic system described above can be usefully complemented by a simplified clinical gait systems which is simply based on a portable data-logger, capable to record accelerometric/inclinometric data coupled with terrain contact information coming from instrumented soles .
| Top |
Literature:
Baratto, L., Capra, R., Morasso, P., and G. Spada (1996) Posturographic imaging: preliminary results of a new method of posturographic analysis. Proceedings of the 10th Conference of the ESB, Leuven, Belgium, August 28-31.
Baratto L., Capra R., Farinelli M., Morasso P., Spada G. (1997) A clinical protocol of movement analysis for the prevention of the risk of falling in elederly patients. Medical & Biological Engineering & Computing, vol.35, Suppl.2, pp. 1289.
Bronstein, A.M., Brandt, T. and M.H. Woollacott (1996) Clinical disorders of balance, posture and gait. Arnold, London.
Katz, E., Downs, T.D., Cash, H.R. and R.C Grotz (1970) Index of independence in activities of daily living. Gerontologist, Part I, 20-30.
Morasso, P. and V. Sanguineti, editors (1997) Self-organization, cortical maps and motor control. Science Elsevier Publ., Amsterdam.
Perrin, P., Lestienne, F. (1994) Méchanismes de l'équilibration humaine. Masson, Paris.
Parmelee, P.A. (1995) Validatino of the Cumulative Index Rating Scale in a geriatric residential population. J. of the American Geriatric Society 43, 130-137.
Tinetti M.E., (1986) Performance-oriented assessment of mobility problems in elderly patients, J. Am. Geriatrics Soc., Vol. 34, pp. 119-126.
| Top | | TIDE 98 Papers |