DO SELF-REPORTED CHANGES IN LIFE SITUATIONS HAVE A
ROLE IN SCREENING FOR INDIVIDUALS AT RISK OF
PARTICIPATION RESTRICTIONS?
P.G. Nicholls*1, Z. Bakirtzief*2, W.H. van Brakel*3, R.K. Das-Pattanayak*4,
G. Norman, M.S. Raju, R.K. Mutatkar*5.
ABSTRACT
This research focussed on the importance of leprosy affected persons' self-reported changes in life situations as indicators of underlying change in participation status as defined by World Health Organisation's International Classification of Functioning, Disability and Health. The authors designed a one-question questionnaire to be used at the primary level to explore recent changes in participation status reported by people receiving treatment for leprosy and assessed its potential as a means to identify individuals experiencing participation restrictions. Primary level workers explored and reported change in the domains of physical status, psychological status, plus changes in relationships with family members, with friends or with community and changes in the ability to work.
Five centres in India participated in the study, collecting data on 197 individuals affected by leprosy. Using the Participation Scale, the authors made baseline and follow-up assessments and recorded self-reported changes at the time of follow-up. Regression analysis demonstrated that self-reported changes in physical and psychological state were predictive of changes in scores on the Participation Scale. So too, were reported changes in the ability to work. Discussion focuses on the potential for a simple screening procedure that would draw attention to individuals experiencing participation restrictions, who may be in need of counselling or rehabilitation interventions.
INTRODUCTION
The present paper is the third in a series of publications concerned with the impact of leprosy and resulting restrictions in social participation. The first publication in the series, describes the development of a scale that measures participation restrictions - the Participation Scale (1). The second describes the development of a screening tool for use at the time of diagnosis to identify individuals at risk of participation restrictions (2). The present paper describes research that assesses self-reported changes as indicators for participation restrictions. The research made extensive use of the Participation Scale and demonstrates its potential as a tool for assessing the status and needs of people experiencing participation restrictions related to leprosy.
The World Health Organisation International Classification of Functioning, Disability and Health defines participation as involvement in a life situation (3). Participation restrictions may occur in any life situation across nine areas of activity and participation. In the context of leprosy, they are recognised as the outworking of the stigmatisation and self-stigmatisation with which the disease has always been associated (4).
The development of the Participation Scale provides field workers with an important tool to assess the impact of leprosy, identifying people experiencing participation restrictions that may be classified as mild, moderate, severe or extreme. It provides information that may guide decisions on the need for interventions, for example, health education, advocacy, rehabilitation or self-care. The present research arose from the suggestion that affected persons' self-reported changes may be important indicators of changes in participation that may signal the need for a more formal assessment using the P Scale, followed by appropriate counselling or rehabilitation interventions. Central to this process would be a one-question questionnaire used by clinic workers at the primary level, to elicit information about recent changes in participation status reported by the affected persons.
This approach parallels the procedures of participatory evaluation, in which the beneficiaries of rural development programmes identify financial, social and personal changes arising from development interventions (5). The approach values the people affected and is responsive to the information they provide.
The objective of the present research, was to field test a one question questionnaire and assess its value in detecting changes in participation restrictions during treatment and follow-up.
METHODOLOGY
The chosen approach for the research, was to conduct baseline and follow-up interviews with persons currently receiving multi-drug therapy for leprosy and to assess the value of self-reported changes as predictors of change, in scores on the Participation Scale. Field- work was conducted by the team involved in the development of the Participation Scale (1).
Inclusion criteria required that participants be affected by leprosy and come from the local control area. Excluded were individuals who were newly diagnosed, or not willing to give written informed consent. Also excluded, were people finding it difficult to communicate, for example, due to a language barrier or mental impairment.
The authors made an opportunistic selection of persons attending out-patient clinics. Baseline interviews were conducted at the first visit after diagnosis and start of treatment. Follow-up interviews were conducted after at least one month. Identification and demographic information was recorded on a purpose-written form and a baseline assessment of participation status was made using the Participation Scale. These were completed in the four months up to August 2003. At the follow-up interview, patients' assessments of recent positive or negative changes resulting from leprosy, were recorded and a repeat assessment of participation restrictions was made using the Participation Scale. Follow-up interviews were completed in late 2003.
Data was entered on computer using EPI-INFO software. From the narrative reported by interviewers, data was coded reflecting relevant positive and negative changes. The authors also coded the details of physical and psychological changes and decisions to conceal the leprosy diagnosis.
For the analysis, Student's t test was used to assess changes in Participation Scale scores between baseline and follow-up and logistic regression analyses to quantify the predictive value of changes reported by patients.
To ensure adequate statistical power for significance testing, each centre in India was asked to complete 40 paired baseline and follow-up interviews. The centre in Brazil was asked to complete 100 interviews, making a total of 300 paired baseline and follow-up interviews. In the event, centres in Brazil were unable to complete fieldwork, so the results presented here are based only on the data received from centres in India. This does result in some loss of statistical power and limits the applicability of the results.
RESULTS
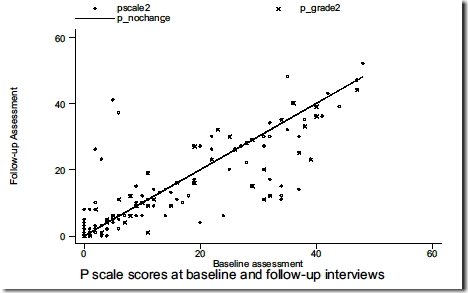
Table 1 summarises Participation Scale scores at baseline and follow-up. There were 197 complete paired assessments. At baseline, 17 individuals (8.6%) were classified as experiencing mild restrictions, 20 (10.1%) as experiencing moderate restrictions and 21 (10.7%) as experiencing severe restrictions. The equivalent figures at follow-up were 18 (9.1%), 22(11.2%) and 16 (8.1%). None of the participants experienced extreme restrictions. Figure 1 presents a scatterplot comparing baseline and follow-up scores, including a line demonstrating no change. There was no statistically significant difference between baseline and follow-up scores, though it is apparent that some individuals experienced important changes during the follow-up period.
Among participants, the WHO Grade 2 disability rate was 74%. In Figure 1, individuals with Grade 2 disability are denoted by "x" while individuals with grades 0 or 1 are denoted by "o". Using Student's t test, no statistically significant difference was found in P scores between WHO grades, or when comparing individuals with grade 2 disability with combined grades 1 and 0. Neither was there evidence of a statistically significant difference in change between baseline and follow-up scores within WHO grades.
Figure 1. Comparison of baseline and follow-up scores from the Participation Scale, including a line denoting no change.
|
|
Follow-up Assessment | ||||
|---|---|---|---|---|---|
| Baseline Assessment |
None (0-12) |
Mild (13-22) |
Moderate (23-32) |
Severe (33-52) |
All |
| None (0-12) |
130 (93.5,92.2) |
5 (3.6,27.8) |
2 (1.4,9.1) |
2 (1.4,12.5) |
139 (70.6) |
| Mild (13-22) |
6 (35.3,4.3) |
6 (35.3,33.3) |
5 (29.4,22.7) |
0 (0,0) |
17 (8.6) |
| Moderate (23-32) |
3 (15.0,2,1) |
5 (25.0,7.8) |
11 (55.0,50.0) |
1 (5.0,6.2) |
20 (10.1) |
| Severe (33-52) |
2 (9.5, 1.4) |
2 (9.5,11.1) |
4 (19.0,18.2) |
13 (61.9,81.2) |
21 (10.7) |
| All | 141 (71.6) |
18 (9.1) |
22 (11.2) |
16 (8.1) |
197 |
|
|
Participation Scale at baseline |
Participation Scale score at follow-up |
Difference in scores |
|---|---|---|---|
| Mean | 11.11 | 10.76 | -0.35 |
| Std Dev | 13.04 | 12.35 | 7.00 |
| Median | 6 | 6 | 0 |
| Maximum | 48 | 52 | 36 |
| Minimum | 0 | 0 | -23 |
Figure 2 presents case studies of two individuals with extreme opposite experiences. The first of these, describes a man who made substantial progress in coming to terms with his disease. He gained in confidence and resumed normal work activities. He developed new hope for the future. His experience was in direct contrast to the experience of the individual in the second case study. This man experienced continuing physical problems and consequent reduction in his ability to write, or to maintain normal economic activities. Early lack of care from the family was no longer a problem, but he retained concerns for his future physical and economic well-being. This led to self-stigmatisation and self-imposed restrictions on social activities. Both these individuals proved able to describe their experiences. The changes they described, are reflected in important changes in scores on the Participation Scale.
|
Person ID 24012 - male aged 35 years - decrease in P score of 23 points Narrative:
Person ID 24022 - male, aged 50 years - increase in P score of 36 points Narrative:
|
Scores on the variables describing self-reported change are presented in Table 2. The most common reports of increased problems relate to the work situation and to the psychological state. These same variables, along with the physical state, were also most commonly reported as improving. The high levels of statistical significance between reported changes and changes in scores on the participation scale, suggest that self-reported changes do provide valid indicators for changes in social participation as measured by the Participation Scale.
| Domain | Direction of change |
N | Median difference in P score |
Statistical significance |
|---|---|---|---|---|
| Any psychological change | Worse Same Improved |
27 150 18 |
0 0 -12.5 |
p<0.001 |
| Any physical change | Worse Same Improved |
12 162 23 |
1 0 -10 |
p<0.001 |
| Any family change | Worse Same Improved |
6 186 5 |
7 0 -15 |
p<0.01 |
| Any friends change | Worse Same Improved |
6 185 6 |
4 0 -15.5 |
p<0.001 |
| Any community change | Worse Same Improved |
8 178 11 |
2 0 -12 |
p<0.001 |
| Any work change | Worse Same Improved |
29 149 19 |
0 0 -12 |
p<0.001 |
| Concealed diagnosis | Worse Same Improved |
181 16 - |
0 -1 - |
n.s. |
Finally, regression analysis was used to explore the association between responses to the change questions and change in participation score (Table 3). This draws attention to the importance of changes in physical and psychological state, as well as changes in the work situation as the primary indicators of a change in participation status. In each case, self- reported problems are associated with an increase in the participation score - that is, increased participation restriction.
|
|
Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| Psychological | -3.50 | p<0.01 | (-6.01 - -0.99) | -3.25 | p<0.01 | (-5.60 - -0.90) |
| Physical | -3.99 | p<0.01 | (-6.72 - -1.27) | -4.43 | p<0.01 | (-7.10 - -1.76) |
| Family | 0.05 | p<0.05 | (-3.88 - 3.99) |
|
|
|
| Friends | -0.68 | ns | (-5.00 - 3.64) |
|
|
|
| Community | -2.06 | ns | (-5.58 - 1.46) |
|
|
|
| Work | -2.13 | ns | (-4.83 - 0.56) | -2.69 | p<0.05 | (-5.29 - -0.09) |
| Concealment | -2.44 | ns | (-5.66 - 0.79) |
|
|
|
|
|
Adj R-squared = 0.3370 | Adj R-squared = 0.3361 | ||||
DISCUSSION
The intention of this research was to assess the value of self-reported change as a predictor of real changes in participation restriction as assessed, using the Participation Scale. Affected persons' self-reported experience of change do have predictive value. Specifically this is true of one's reported changes relating to one's psychological state, to one's physical state and to changes in the ability to work. This suggests that a basic screening process that recorded self-reported changes in key life areas may have value in identifying individuals at risk, or already experiencing participation restrictions. The design of the proposed tool is presented in Figure 3. Such a tool might be used in the context of health service delivery, or as part of a rehabilitation programme. It would make only limited demands on staff time and skills. Its adoption in the field situation would require that individuals reporting negative changes receive appropriate assistance in the form of counselling, home visits or rehabilitation interventions.
| Screening for self-reported changes in participation status |
|---|
|
Has leprosy caused any change in your life since your last/recent visit? Yes/No If any positive or negative changes, please explain: All responses should be followed up by the following exploratory questions: Any positive or negative changes in your physical state? Yes/No If yes, please explain: Any positive or negative changes or impact in your family? Yes/No If yes, please explain: Any positive or negative change or impact among your friends? Yes/No If yes, please explain: Any positive or negative change or impact in your community? Yes/No If yes, please explain: Any positive or negative change or impact in your work? Yes/No If yes, please explain: |
|
Note changes that have occurred: Positive changes: Negative changes: |
|
Note actions to be taken: Referral to social/rehabilitation worker for assessment Yes/No Provided advice Yes/No Arranged home visit Yes/No No current action but follow-up at next MDT visit Yes/No |
The basic design of this screening tool may be of wider application, for example, in the context of other chronic stigmatised conditions such as HIV/AIDS.
CONCLUSION
The present research has confirmed the importance of self-reported changes as indicators for real changes in participation among people affected by leprosy. Self-reported psychological and physical changes have predictive value, as do reports of changes in the ability to work.
The research provides evidence that screening self-reported changes may be effective in drawing attention to individuals requiring some form of counselling or rehabilitation intervention. The screening process may be adopted in the context of other stigmatised conditions.
*1 Address for correspondence
School of Nursing and Midwifery
University of Southampton
Highfield, Southampton, SO17 1BJ, UK
e-mail:p.nicholls@soton.ac.uk
*2 Postbox 1527, SP 18041 - 970, Sorocaba
Sao Paulo, Brazil
*3 KIT Leprosy Unit, Wibautstraat 137 J
1097DN Amsterdam, The Netherlands
*4 The Leprosy Mission Research Resource Centre
Shahadara, Nanda Nagari, Delhi 110095, India
*5 Medical Anthropology, School of Health Sciences
University of Pune, Pune - 41007, India
ACKNOWLEDGEMENT
The authors wish to express their sincere gratitude to the people who agreed to be interviewed about often painful aspects of their lives. We are very grateful for the hard work, enthusiasm and dedication of the team involved in field work relating to the development of the Participation Scale: Mr. Ishwor Khawas, Dr. Annamma John, Dr. Harveen Das, Dr. Loretta Das, Mrs. Ratna Philip, Dr. Robins Theodore, Mrs. Eben Baskaran and Dr. Geetha Rao. We are very thankful to the Participation Scale Advisory Group, consisting of Dr. P.K. Gopal, Dr. Ulla- Britt Engelbrektsson and Mrs. Valsa Augustine, who provided wisdom, experience and encouragement to the team.
We are indebted to the sponsors of the research programme, the International Nepal Fellowship, The Leprosy Mission International, the American Leprosy Missions and the German Tuberculosis and Leprosy Relief Association. We thank Dr. Cornelius S. Walter, TLM Director for South Asia, for his support of the work carried out in India.
REFERENCES
- Van Brakel WH, Anderson AM, Mutatkar RK, Bakirtzief Z, Nicholls PG, Raju MS, Das-Pattanayak RK. The Participation Scale: Measuring a key concept in public health. Disabil Rehabil. 2006;28:193-203
- Nicholls PG, Bakirtzief Z, Van Brakel WH, Das-Pattanaya RK, Raju MS, Norman G, Mutatkar RK. Risk factors for participation restriction in leprosy and development of a screening tool to identify individuals at risk. Lepr Rev. 2005;76:305-15.
- World Health Organisation. The International Classification of Functioning, Disability and Health. Geneva: World Health Organisation, 2001.
- Bainson KA, Van den Borne B. Dimensions and process of stigmatization in leprosy. Leprosy Review 1998;69(4):341-50.
- Chambers R. Whose reality counts? Putting the last first. London: Intermediate Technology Publications, 1997.