DESIGN AND PRODUCTION OF
SPECIFIC DEVICES
A. Lower-limb prostheses
Below-knee amputations are the most common type of amputation; above-knee amputations are the next most common. To produce below-knee (BK) prostheses, a production unit must have the necessary parts, such as pylons and prosthetic feet, and the facilities and expertise to make sockets and shanks. The basic components of a BK prosthesis are the socket, the shank and the foot-ankle system. A shank is a structural component of a prosthesis which connects the socket to the foot-ankle system and transfers the load of body weight to the foot and the floor.

There are two types of prostheses: exoskeletal (or crustacean) and endoskeletal. Exoskeletal prostheses are the most commonly used in the region. Their shanks are on the outside, typically made of wood, thermoplastic or polyester resin. The inside is usually filled with wood. Endoskeletal prostheses have the most lifelike appearance, but require careful maintenance. Their shank is on the inside. It is a central tube, called the pylon, which is usually made of aluminum. It is covered in foam or polypropylene and encased in a latex or fabric stocking for cosmetic purposes. These prostheses are available in many developing countries of the ESCAP region, although they are all imported.
Three different materials are most commonly used in the making of BK prostheses: aluminium alloys, polypropylene and titanium. Polypropylene has three advantages over aluminium: it is much lighter; it is cheaper; and setting up production facilities may be easier for it than for aluminium.
Titanium is extensively used in China for making expensive high-quality pylons, which are attached to the prosthetic foot and socket through an attachment plate. This considerably increases the strength and reduces the weight of a prosthesis. Fabrication of titanium parts is difficult, however, as special equipment is required to process the metal in an oxygen-free atmosphere.
Some countries, including Thailand and Viet Nam, have attempted to use computer-aided socket design and manufacture. The main difference is that the computer-aided technique does not require that a plaster-of-Paris (POP) cast of the stump be taken and a negative mould be produced in order to make the positive mould. Instead, a positive POP cast is directly made by digitizing the shape and the size of the stump through computerized scanning. Unfortunately, the expertise needed to use the method is not yet widely available in developing countries of the ESCAP region, and so the application of the technique has thus far had limited success.
The alignment of prostheses and orthoses should ideally be established by well-trained professionals. However, most Asian and Pacific developing countries do not have sufficient numbers of trained prosthetists to establish alignment in this way.


The most common BK prosthesis now in use is the patellar-tendon-bearing (PTB) prosthesis. The shank of a PTB prosthesis is usually made of wood, but its socket is made of polyester resin or (increasingly) polypropylene. The socket is made using a mould based on a plaster cast of the stump. (See the Technical Specifications Supplement for further details.)
The Jaipur prosthesis, a type of exoskeletal prosthesis which was originally made of aluminium, has a socket that is open on both ends. This makes it easier for the prosthesis to fit stumps of non-optimal size, common in Asian and Pacific developing countries. Its open socket is also more suitable for hot climates than a total-contact socket. It is, however, less suitable for wet climates where water and moisture can enter. Jaipur prostheses generally include a Jaipur Foot as their foot component, although some Jaipur prostheses use different kinds of feet.
People cured of leprosy should not receive a prosthesis with this type of open-ended socket. As peripheral anaesthesia often extends up to the knee, they need a perfect fit that does not require sensory feedback. (See Box 7 for further detail.)
The initial work on providing prostheses in Cambodia started with an aluminium Jaipur prosthesis. An NGO in Thailand provides these aluminium prostheses through a mobile workshop in rural and remote areas.
The aluminium Jaipur prosthesis remains the least expensive and the easiest to produce. It does, however, have some major drawbacks. First, it is less physically attractive than most other prostheses. Second, as aluminium absorbs heat, many users in a hot climate find it too hot to be comfortable. Third, the fact that it is produced manually makes alignment difficult. It is far easier to adjust the alignment of modular, endoskeletal prostheses. Poor alignment can, in turn, make it awkward to walk with this prosthesis. As a result of these difficulties, few agencies in Cambodia and Thailand still make it.

The design of the Jaipur prosthesis has been considerably changed by using high-density polyethylene (HDPE) to make both the socket and the shank. The HDPE is available in the form of pipes designed for irrigating rice fields. It is thus easily available in many developing countries in the region. The Technical Specifications Supplement provides detailed instructions on how to make the HDPE Jaipur prosthesis. Although the HDPE prosthesis is generally an improvement over the aluminium design, it requires an oven and a facility for taking a plaster cast, which the aluminium prosthesis does not.
The conventional above-knee (AK) prosthesis is made of willow wood, with a socket carved in a wooden shank. This type of prosthesis is still in use, but the number of users is quickly decreasing. Its heavy weight is a disadvantage. The newer thermoplastic or resin prostheses are lighter and easier to make.
The shape of the socket is crucial for comfort and functionality. The socket should allow blood circulation without being loose. Quadrilateral sockets are nearly rectangular in shape when viewed from the top. They are among the most commonly used sockets in the region, as they provide almost total contact with the limb.
For active amputees with good blood circulation, a close fit between the stump and the socket can create a suction that holds the prosthesis in place. In this kind of socket, called a suction socket, nothing is worn on the stump. When blood circulation is poor, a sock is worn over the stump and the socket is held in place by a belt around the pelvic area. This latter type is the most common type of socket in the region.
B. Upper-limb prostheses
In most Asian and Pacific developing countries, only a few rehabilitation centres produce prostheses for upper limbs (arms and hands).In Afghanistan, for example, upper-limb prostheses are not provided except when a user requests one for cosmetic reasons or for young bilateral upper limb amputees to enhance functional independence(15).

The basic components of an upper-limb prosthesis are:
- (a) Socket;
- (b) Wrist unit;
- (c) Terminal device or hand;
- (d) Power transmission system;
- (e) Forearm;
- (f) Arm section;
- (g) Elbow mechanism (for above-elbow amputees);
- (h) Suspension system.
Leather or nylon cords transmit tension force, generated by movement of the shoulder, to operate the terminal device or the hand. The elbow is not always needed, as prostheses are most commonly prescribed for people with below-elbow amputations, whose elbow function is retained. The function of the suspension system is to hold the prosthesis in position during all of its possible movements.
The terminal device is a centrally important part of the prosthesis, since it provides replacement of the limb's most important function, prehension or ability to grasp an object. The hand is one of the most intricate organs of the human body. As such, it poses a serious challenge to the designing of prostheses meant to replace the function of hands. Nobody has yet designed an artificial hand which even comes close to replicating a human hand. Commercially available artificial hands typically have only the ability to open and close, with little other freedom of movement.
Generally, replacement hands and terminal devices are of two types: functional or cosmetic. The most frequently used cosmetic versions can neither open wide enough to hold many common objects nor flex tightly enough to hold small objects in a firm grip. This limits their functional range.
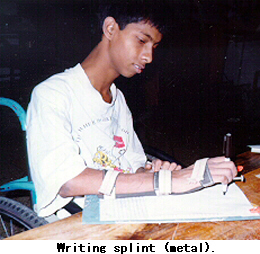
Functional hands are strong and sturdy mechanical hands, to which different types of terminal devices can be affixed. The terminal devices are designed so that one end of the terminal device fits easily into the small socket made in the prosthetic hand. The terminal devices are usually made of steel. A voluntary opening hook, which can be opened or closed whenever the user choses to do so, is one of the most commonly preferred terminal devices. Artisans, farmers and agricultural labourers can use these functional hands effectively for both farm and non-farm work, including ploughing the field, digging the ground, carpentry and welding.
The most commonly used hands are rigid hands and cosmetic hands. Presently, the most successful arrangement has been to operate the first and second fingers along with some motion of the thumb, in a three-jaw-chuck type of prehension pattern. Mechanical hands with finger phalange movement, which improves prehension, are also available in Asian and Pacific developing countries.
A manual worker will likely require a functional hand to replace even a non-dominant hand. For others, a cosmetic hand will likely be an adequate replacement, at least for a non-dominant hand. Unilateral amputees generally find it easier to learn to use their non-dominant hand than to use a functional prosthetic hand. Bilateral amputees are often best served by one functional hand with a hook as a terminal device and one cosmetic hand.
A hand prosthesis can be activated and operated either through body power or through an external power source (e.g., batteries). Myoelectric hands, operated through contact with electrodes in the socket, are popular in developed countries. They are used in a few countries in the region, including China, but their long-term usefulness has yet to be established and their cost is often high.
Currently, the only manufacturer of electronic hands in an Asian or Pacific developing country is the Nevedac Prosthetic Centre at Chandigarh, India. The Nevedac Centre's electronic hands, with switch-control systems, are made from indigenous materials. They are cheaper than myoelectric hands but just as effective. The Centre has also developed mechanical hands which allow all five fingers to move. People from afar have come to obtain these hands.
C. Orthoses
Orthoses are also known as calipers or braces. Although a brace is generally considered to be larger than a caliper, the two terms are often used interchangeably. This review uses only the more general term orthosis to avoid confusion.
Orthoses have two major purposes: first, to support or maintain a weak limb; and second, to help prevent or correct future deformities and contractures.
Only a few developing countries of the ESCAP region have paid substantial attention to the production of orthoses, in spite of large numbers requiring them. India has addressed the need for orthoses in response to the consequences of polio among many people. In those countries which produce orthoses, manufacturing capacities are not completely used.
A combination of hip knee ankle foot orthosis (HKAFO) and crutches has been used effectively by the Christian Medical College in Vellore, India, for rehabilitating paraplegic people in their own village surroundings (see Field Visit Notes in Madras Workshop Proceedings). Unlike most wheelchairs, this combination permits them to work in the field and thus remain productive members of their families, as well as allowing for regular exercise.
Metallic orthoses are the most common type of orthosis in developing countries of the ESCAP region. Conventional metal lower-limb orthoses require the use of special shoes. These shoes are user-specific, so full orthoses can only be produced at a clinic or hospital with trained prosthetic and orthotic technicians. The special leather shoes required are made in the rehabilitation workshops to suit the size and condition of the user's foot. For example, the inside height of the shoe may have to be increased to account for limb shortening.


Unfortunately, many countries face a shortage of shoemakers. For this reason, India's rural programme attempted to use wooden clogs in place of leather shoes. However, these clogs were unstable, unattractive (because both feet and clogs became dirty quickly) and came loose after continuous use. As a result, users did not accept them.
For a child who needs a below-knee orthosis, a thermoplastic orthosis moulded to fit the child's leg and foot has these advantages:
- (a) It weighs less and is often more comfortable than metal orthoses;
- (b) It can fit the child comfortably and exactly (if made well);
- (c) It is not prone to corrosion and can be worn easily with ordinary shoes.
The fit of thermoplastic orthoses, however, is very close, and this often makes them feel uncomfortably hot in tropical climates. In addition, a casting must be made, which increases the complexity of the production process.
Even if a better design of thermoplastic orthosis existed, the limited availability of thermoplastics and the need for the related equipment would remain a deterrent to their use, especially in rural areas. Furthermore, thermoplastic orthoses are not yet produced in a modular way, so a rehabilitation centre will need in-house moulding facilities to produce them.
Finally, thermoplastic orthoses may not be suitable when, as a result of the type of disability faced, orthoses have to bear high loads and be very stable. In such cases, orthoses made of thermoplastic and metal may be the best option.
The hybrid of thermoplastic and metal will likely become the favoured material, as it has the advantages of both thermoplastic and metal. Such an orthosis is being prescribed in many places. However, it does require different machines, tools and technical skills in rehabilitation centres. It is easier for those centres to deal only with the technology required for one material.
The thermoplastics usually used for making orthoses are polypropylene and polyethylene. The strength of thermoplastic orthoses is insufficient to withstand the tough loading conditions imposed by the rough terrain and usage pattern in rural areas, such as when feet hit an obstacle and get bent in one direction. Glass-filled polypropylene has been used to overcome this problem, but it is expensive. Another solution is to include an aluminium support and aluminium knee joint in a polypropylene orthosis.
In India, for people with good biceps muscles and hand- on-knee gait, floor-reaction orthoses (FRO) have been found useful. An FRO is designed so that the toe strikes the ground first; the reaction force from the ground pushes back the knee, making it stable. As a result, users do not require a hand-on-knee gait. Some rehabilitation centres also use PVC pipes (which are used to carry water and are available locally) to produce orthoses.

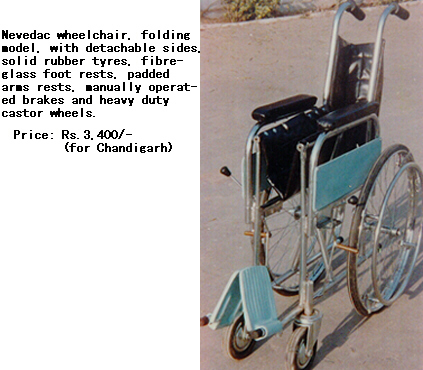

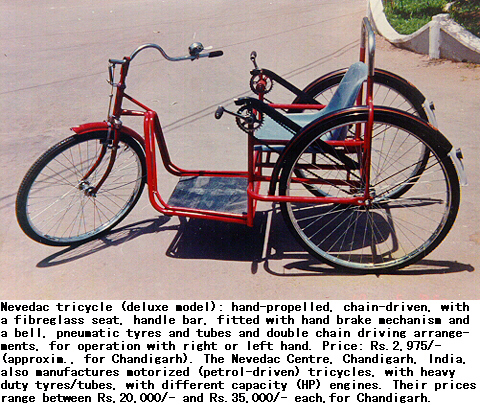
Source: All Nevedac items were contributed by Colonel D.S. Vohra, Director, Nevedac Prosthetic Centre, Chandigarh, India.
D. Wheelchairs and ground mobility devices

Wheelchairs in developed countries often use high-technology materials like aluminium alloys, titanium and carbon fibre. The cost of such wheelchairs, however, is usually unaffordable by most users in Asian and Pacific developing countries. Non-availability of spare parts and maintenance facilities are additional drawbacks. As a result, steel is predominantly used for fabricating wheelchairs in the developing countries of the region. Aluminium alloys have recently been used for making wheelchairs in Thailand (see Box 6). These wheelchairs, however, are only suitable for movement on smooth surfaces.
NGOs in Cambodia use a wooden wheelchair (see Technical Specifications Supplement). Compared with metal wheelchairs, wooden wheelchairs are stronger and easier to repair and adapt in rural areas. They were initially cheaper as well, although this advantage has faded with rises in the price of wood.
The design of wheelchairs used in Asian and Pacific developing countries has often been based on specifications intended for people in other regions of the world. These wheelchairs are often oversized. The width and depth of the seat and the height of the armrests are unsuitable for and unacceptable to their users.
Some wheelchairs in use in the region, especially those provided free of charge to users, were designed for use in institutions, especially hospitals even though the actual use of the wheelchairs is in daily life. Such wheelchairs have many problems including:
- (a) Inappropriate size;
- (b) Difficulty of controlling the chairs;
- (c) Poor facility for transferring in and out of the chairs;
- (d) High cost;
- (e) Unsuitability for rural use;
- (f) Lack of durability;
- (g) Difficulty and expense of repairs.

Jesuit Service Cambodia, an NGO, and the MacKean Rehabilitation Centre in Thailand, use a stronger castor wheel assembly, but feedback from users is not available. It is, however, clear that wheelchairs for use in rural areas have to be durable and sturdy. Wheelchairs for distribution to the rural poor must be redesigned to fit their lifestyles.
Most wheelchairs produced in the region have the conventional configuration of two castor wheels in the front and two main wheels in the back. An exception is a wheelchair made in Cambodia that has only one castor wheel in the front.
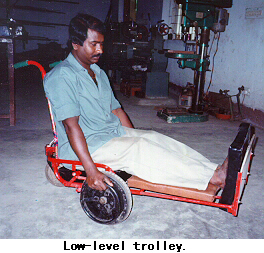
Ground mobility devices, or low wheelchairs, are similar to wheelchairs, but work at ground level rather than at chair level. They can be more useful than wheelchairs in places where many tasks are performed close to ground level, especially in rural areas. Such tasks include food preparation, welding, praying, eating, masonry and craft work. The ground mobility device developed by the National Institute of Design in Ahmedabad, India, with contributions from the International Centre for the Advancement of Community Based Rehabilitation (ICACBR), was designed with the participation of women with disabilities and field tested by them. (See the Technical Specifications Supplement for descriptions of the parts and process required to produce the device.)
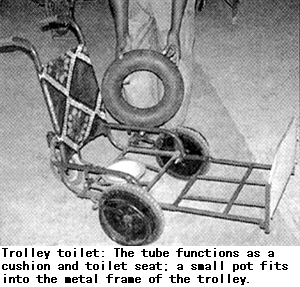
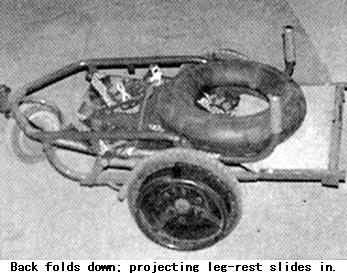
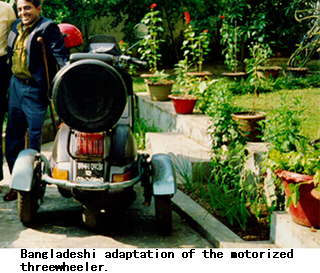
The Centre for the Rehabilitation of the Paralysed in Bangladesh has developed a similar ground-level trolley device(18).The user sits on soft coconut fibre placed over an air-filled inner tube (from a scooter). The inner tube serves both as a cushion and as a toilet seat. A small removable pot fits into the metal frame of the trolley and is centred under the hole in the tube. The trolley is collapsible. Its back folds down and the projecting leg-rest slides in.
Wheelchairs are mass-produced in a number of countries, including Bangladesh, Cambodia, China, India, Pakistan, Thailand and Viet Nam. In China, about 100,000 wheelchairs are produced per year. These are produced in 20 factories, some owned by the Government and some privately. Of these, ten produce wheelchairs solely for export.
In Cambodia and Malaysia, bilateral above-knee amputees have been provided wheelchairs in their workplaces. Many of these amputees are engaged in tailoring in vocational centres in Malaysia and in machine shops in Cambodia.
Armenia currently imports all its wheelchairs, but its Ministry of Social Welfare has begun a project to have wheelchairs, especially for children, made locally through the Yerevan Prosthetic Orthopedic Enterprise.
E. Tricycles and adapted motorcycles

Many wheelchair manufacturers in developing countries of the ESCAP region also produce tricycles. Tricycles are devices with three main wheels; they are larger than wheelchairs but operated in similar ways (by hand, electricity or petrol). They are useful for long-distance mobility. In several developing countries of the region, tricycles have enabled people with disabilities to work far from their homes. A tricycle can also be used for carrying extra loads, such as groceries or household items. People in rural areas often prefer tricycles to wheelchairs because tricycles are sturdier and can more easily negotiate rough terrain.
Tricycles, however, have some drawbacks. A tricycle cannot replace a wheelchair for indoor and around-the- house mobility, as there will likely be insufficient space. Moreover, as tricycles are heavier than wheelchairs, users must have enough muscle power in their hands and upper bodies to propel manual tricycles.
For meeting different needs, many people with disabilities need both a wheelchair and a tricycle. In Cambodia, an attachment has been designed which makes it possible to convert a wheelchair into a tricycle. Jesuit Services Cambodia produces this attachment on a regular basis.

The most common configuration of tricycle is one wheel in the front used for steering and two main (rear) wheels which are attached to, and moved by, a chain or a hand lever.
The Shanghai Wheelchair Factory makes the best-selling manual tricycles in China, at market prices between US$70 and US$140. Three models, in different sizes, are driven with only one hand; the other hand is for direction control. A fourth model, the SJ26Q, can be driven by two hands or two feet. When two hands drive it, they also control direction. Although minor repair of these tricycles can be performed at bicycle repair sites, some parts can only be obtained from the manufacturers, which makes major repair difficult and inconvenient.
It is also possible to produce a petrol-driven motorized tricycle similar to a motorcycle. About 20,000 motorized tricycles are produced in China each year. The market prices for such a motorized tricycle are between about US$410 and US$720. The most popular model is Model CJ50ZC manufactured by Chongqing Jialing Industry Co. Ltd.
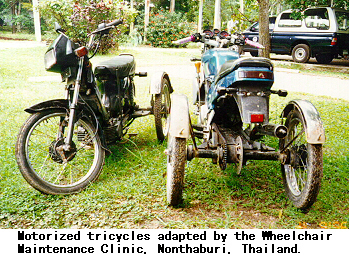
A motorcycle modified and adapted to fit the needs of wheelchair users can be an important assistive device which provides users with mobility over long as well as short distances. The cost of such a device is, however, high. Furthermore, in some cases, government action has hindered more than helped their production. Not only is such adaptation rarely if ever subsidized, but in some countries, including Thailand, it is actually illegal to produce and drive an adapted motorcycle. This illustrates the importance of flexible regulations and the problems of imposing legal sanctions for violating quality-control standards and procedures.
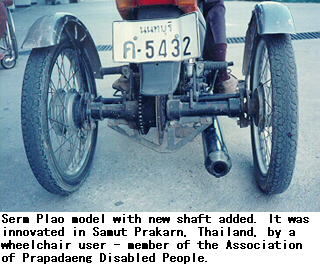
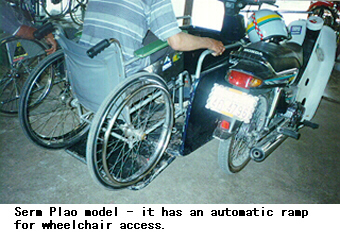
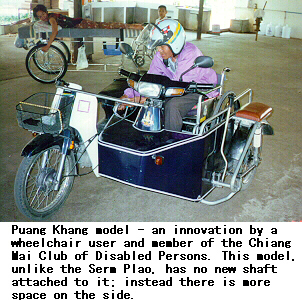
In Thailand, there are two popular designs of this adaptation. The first places a bay at the side of the motorcycle onto which a wheelchair can be ridden, facing forward. The handlebars are moved to the wheelchair user's focal point and the transmission, normally operated by foot pedal, is operated with a lever. This modification costs 6,000-7,000 baht(20), in addition to the cost of the motorcycle.
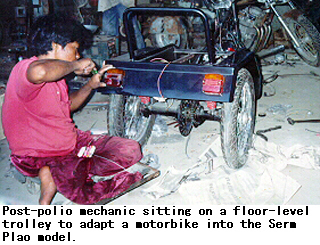
The second modification, known as the Seum Plao, produces a result similar to the Chinese design for a motorized tricycle. The user sits in the middle of the vehicle, which makes the modification stronger, safer, and more stable. However, this design requires a modification of the cylinder, which is difficult and involves more sophisticated mechanical skills. As a result, the cost of the modification is about 12,000 baht (US$330).
Source: All items on this page were contributed by Colonel Topong Kulkhanchit, APHT, Thailand.
F. Devices for people with visual impairments
Most devices for blind people are not highly user-specific. It is therefore easier to mass-produce devices for blind people than most devices for people with locomotor disabilities. Nevertheless, decentralized production has the advantage of facilitating distribution. The ease of decentralized distribution and the (potentially) lower costs of mass production should be carefully weighed while deciding on a production strategy.
Devices for people with visual impairments range from simple mechanical tools to sophisticated computerized devices. Most Asian and Pacific developing countries do not produce devices like white canes and braille slates despite the simplicity of such devices.
Speech synthesizers are an important device for the education and employment of people with visual impairments. Most speech synthesizers currently in use are available only in English. Speech synthesizers have been produced in India using speech chips available from Japan, Taiwan Province of China, and the United States of America. Such chips are expensive, however, and a more recent policy is to use special software developed for use with the sound blaster-compatible sound cards readily available in the market.

Thailand has developed a package for optical character recognition of the Thai language. This will likely empower many people with visual disabilities to access better educational and employment opportunities.
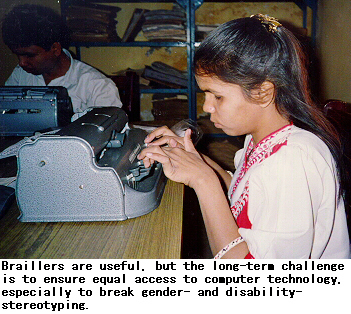
Many countries import their mechanical braillers, braille shorthand machines and computerized braille embossers from developed countries. Braillers have been produced in India for many years. China now makes braillers and all their parts locally.
Low-speed computerized braille embossers based on indigenous designs and locally available parts are now produced in India. These embossers are useful in classrooms and other situations where the workload is not heavy. Prices of these locally produced embossers are lower than the prices of similar imported devices. Closed-circuit television systems with magnifying facilities are also produced in India.
Thermoplastic braille writing frames are produced in China, India and Thailand. The frames made in China and Thailand are four-line frames, i.e., the frame has to be moved after each four lines that the user writes.

Braille frames can save on consumption of braille paper if they can also perform interpointing writing, i.e., braille writing which uses the space between two dots for writing on the reverse side of a page, allowing both sides of the page to be used. A 26-line interpointing writing frame developed in India is now produced there on a regular basis. This is made from locally available plastic material.
To produce braillers and braille writing frames in large numbers, accurate dies must be designed and produced so that the devices can be produced using an injection-moulding process. Metallic devices are generally being replaced with plastic ones because of the tremendous saving in weight, and because of increasing availability of good injection-moulding facilities for making the plastic parts. Forging and machining are essential for metallic parts, such as levers and keys used in braillers or facilities for casting.
G. Devices for people with hearing impairments
Few developing countries in the ESCAP region produce hearing aids. The exceptions are China and India, both of which produce many types of hearing aids. China has set up joint ventures with foreign companies for the production of hearing aids. In India, on the other hand, all the companies making hearing aids are domestic ones. The hearing aids are produced according to Indian standards, which are similar to international standards.
Producers of hearing aids generally do not produce their own parts, but obtain them from other sources. The production techniques, which are similar to those used to produce electronic audio systems, require trained engineers and technicians.
Many useful devices other than hearing aids are neither produced nor imported by most Asian and Pacific developing countries. These include group hearing aids, telephone amplifiers, inductive couplers, vibrating indicators, TV listening devices, telephones with flashing lights, vibrating alarm clocks, FM hearing aids and loop induction systems.
15. Thomas Berhane, "Sandy Gall's Afghanistan Appeal: Orthopaedic Workshop and Physiotherapy Programmes for Afghans", in Report of ISPO Consensus Conference on Appropriate Prosthetic Technology for Developing Countries, Phnom Penh, June 5-10, 1995.
16. See the Technical Specifications Supplement for information on the process of making orthoses.
17. R. Saha and others, "Study of Wheelchair Operations in Rural Areas Covered under the District Rehabilitation Centre (DRC) Scheme", Indian Journal of Disability and Rehabilitation, July-December 1990.
18. David Werner, Nothing about Us without us, p. 194. HealthWrights, Palo Alto, U.S.A., 1998).
19. For information on the tools required to make wheelchairs, see Ralf Hotchkiss, Independence through Mobility: A Guide to the Manufacture of the ATI-Hotchkiss wheelchair Appropriate Technology International. Washington, DC,
20. Equivalent to approximately US$150-200 in September 1997.
Box
Box 7: Devices for People Affected by Leprosy
Leprosy has two aspects: loss of motor function and loss of peripheral (protective) sensation. Loss of sensation means that people with leprosy cannot sense heat or pain from mild injuries, and sometimes even severe ones. As a result, they must exercise special care and use protective coverings, handles and clothing. The injuries that go unnoticed can easily become infected. If these injuries are not attended to in time, they may lead to the loss of fingers and toes. The loss of these motor functions makes it difficult for people affected by leprosy to engage in many productive activities.
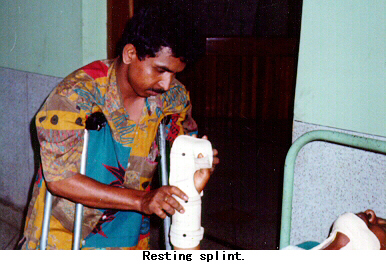
Oven gloves, conventional gloves and mittens can protect hands from injury. Therapeutic splints are made to correct contractures of the inter-phalangeal joints as an aid to mobilizing exercises, massage and other physiotherapy procedures. These splints are made with polyvinyl chloride (PVC) sheets and velcro straps. Some rehabilitation programmes also use soft PVC hose pipes, which are cut lengthwise into two slightly curved gutters. These gutters are attached using velcro straps, sticking plaster or bandages.
People cured of leprosy who have "foot drop" require functional devices to achieve a normal gait. Foot-drop spring shoes are helpful until a surgical correction is carried out. Protective devices are critical for feet without sensation because the foot is the body part most vulnerable to injury.
Footwear should fit closely without being tight. Socks are necessary to reduce the frictional trauma from the upper portion of shoes. Leather is a good material to use in shoes for people with leprosy or cured of it, because it absorbs sweat and moulds itself to make a better fit over time. Since many people affected by leprosy are poor, however, they cannot afford leather shoes.

(Source: Schieffelin Leprosy Research and Training Centre and Hospital, Karigiri, Tamil Nadu, India.)
Box 8: The Wheelchair Maintenance Clinic, Nonthaburi, Thailand

Topong Kulkhanchit, as a wheelchair user himself and as President of the Association of the Physically Handicapped of Thailand (APHT), was dissatisfied with the standard institutional design of wheelchairs and the poor facilities available for their repair and maintenance. Mr. Topong and his friends decided to start a project to make new wheelchairs better suited for active lifestyles and to provide a proper maintenance service. Today, the Wheelchair Maintenance Clinic has an all-in-one programme covering the production, repair, and maintenance of wheelchairs, and training in all of these functions.
In 1991, Mr. Topong and his friends proposed such a project to the Asahi Shimbun Social Welfare Organization of Japan. Asahi Shimbun agreed to ship 100 renovated used wheelchairs from Japan to Thailand every year from 1993 to 1995, if the APHT would be responsible for customs procedures, local transportation, storage, distribution, and most importantly, maintenance. Since 1995, the APHT Wheelchair Maintenance Clinic has been able to develop and produce its own wheelchairs. Acting on a suggestion of Mr. Topong, Asahi Shimbun now ships wheelchairs to Bangladesh and the Philippines.
In 1993, the APHT sent two staff members (with disabilities) to Oita Taki Corporation in Japan for a month of training on wheelchair maintenance. In the following two years, these staff members were able to train many other local technicians. Some of those trainees now work at the Clinic. By 1996, the training became a TCDC programme, with people with disabilities from Bangladesh, the Philippines and Viet Nam joining its training course. In 1997, the trainees included two from Bangladesh, two from the Lao People's Democratic Republic, two from the Philippines, and three from Viet Nam, as well as 21 from Thailand. Every trainee builds at least one wheelchair during the course. Trainees acquire the skills to repair and maintain bicycles as well as wheelchairs.
The main Clinic in Nonthaburi sends most spare parts, free of charge, to provinces in Thailand where its trainees are working. This frees the provincial chapters of the Clinic from having to charge people in their communities. The Clinic operates 24 hours a day, seven days a week, with spare wheelchairs available on loan while regular wheelchairs are fixed.
Box 9: Wheelchair TCDC outcome in the Philippines
Following their training at the Wheelchair Maintenance Clinic, Thailand, and further short-term training in Japan, a small wheelchair workshop was set up in Cebu City, Philippines, by one of the Filipino participants.
Four wheelchair users are employed at the workshop run by an organization of persons with disabilities, Handicapped's Anchor is Christ (HACI), Inc. Two of the workers had been trained in welding in the National Manpower and Youth Council, Cebu City. HACI had negotiated for their admission to the welding course. It had also mobilized funding for their training materials, as well as for subsidies for their daily transport and food.
A donation of equipment amounting to US$2,000 enabled the HACI workshop to commence production, using a Japanese wheelchair design.
Similar wheelchair workshops run by persons with disabilities also exist in Bacolod, Davao and Manila.
The HACI workshop is just one year in existence. It produces three types of wheelchair: stainless steel (Pesos 11,000), chrome-plated (Pesos 9,000) and painted (8,000). The castor wheels are imported from Taiwan Province of China. Seven wheelchairs are produced each month.


Box 10: Making Use of Low Vision

People with low vision are often treated as blind, for a number of reasons. The first problem is a lack of knowledge and understanding about low vision. Second is a lack of appropriate low-vision training. The third problem is a lack of assistive devices. Assistive devices can aid some of these "blind" people to make effective use of the residual vision they have, so that they can, for example, read ordinary writing rather than braille. Unfortunately, the limited availability of optical magnifying components, such as lenses, means that large numbers of people in Asian and Pacific developing countries remain handicapped.
WHO data estimates that one per cent of people in India, 0.6 per cent in China, and 0.8 per cent in the rest of the Asia-Pacific region were blind in 1990, a total of about 21.4 million. The estimate of people with low vision, by contrast, is about 1.9 per cent.
Go back to the Contents
ECONOMIC AND SOCIAL COMMISSION FOR ASIA AND THE PACIFIC
Production and distribution of assistive devices for people with disabilities: Part 1
- Chapter 3 -
Printed in Thailand
November 1997 1,000
United Nations Publication
Sales No. E.98.II.F.7
Copyright c United Nations 1997
ISBN: 92-1-119775-9
ST/ESCAP/1774