DESIGN AND PRODUCTION
OF PARTS
The success of a production strategy for finished assistive devices inevitably depends on the availability of their parts. Some parts, such as castor wheels in wheelchairs, are subsystems, i.e., they act as one unit, but contain other parts within them. Many parts useful in the production of assistive devices (e.g., ball bearings and wheelchair tyres) are already produced in developing countries of the ESCAP region for incorporation in other domestic products such as bicycles.
A. Prostheses
Many countries, including Bhutan, Fiji, Malaysia, Maldives, Nepal, Sri Lanka and Thailand, import parts for prostheses from within and outside of the region.
A strong system of local production of parts for prostheses now exists in several developing countries of the ESCAP region.
Cambodia's well-developed system for producing prosthesis parts is based on the assistance of international NGOs providing rehabilitation services. In Cambodia, most parts for lower-limb and upper-limb prostheses are manufactured by one international NGO, the International Committee of the Red Cross (ICRC). The parts are made of polypropylene (sometimes recycled), aluminium and steel. Most raw material is imported. The production is carried out in a factory with modern facilities for vacuum forming, injection moulding, welding, stamping and milling.
The parts used were designed at the ICRC Headquarters in Geneva, Switzerland, which produces, according to its international specifications, the dies and moulds used in Cambodia. There are now attempts to have the dies made locally. In the past few years, the factory has adopted a more uniform production process, substantially reducing the production cost and time.
In India, most parts for prostheses are manufactured by a government-owned factory, Artificial Limb Manufacturing Corporation (ALIMCO). ALIMCO was set up in the 1970s using foreign technology and knowledge, but today the company is totally self-reliant. This self-reliance has been achieved by recruiting qualified local engineers to manage the industry. ALIMCO has also developed new methods of production and quality control.
China uses a variety of strategies for the production of prosthesis parts. It produces most parts locally, but also imports some high-technology parts, such as high-performance prosthetic feet. China produces about 50,000 foot pieces made of rubber and wood in three Government-owned factories.
The knee system of an AK prosthesis is the part that most distinguishes producing an AK prosthesis from producing a BK prosthesis. The knee system includes the artificial knee and the mechanism that links it to the shank; the knee, in turn, includes the knee joint and its enclosure.
The knee system is crucial for an AK prosthesis user, as it determines the types of activities that she or he can undertake. Daily life in many countries and areas of the ESCAP region involves ground-level activities such as food preparation, washing, eating, praying, welding, masonry and craft work. A knee system must therefore allow for rotation of the limb and flexing of the foot in a way that permits sitting and squatting on the ground.
To provide a normal appearance during walking, the knee joint should not buckle as the amputee rolls over the artificial foot during the stance phase of walking. This is achieved by using mechanical friction around a bolt that connects the socket to the thigh. The bolt is located behind the path of the weight of the body so that it will not buckle when the user is standing straight.
The single-axis joint, so named because it can move around only one axis, is the most commonly used knee joint because of its simplicity and low cost. One of the joint's limitations is that its appearance is normal during walking at only one walking speed. Its users must be careful while walking, especially on uneven ground, to avoid stumbling. Other types of joints exist, such as the polycentric knee joint, but they are expensive and difficult to repair and maintain. As a result, they are not widely used in the region.
The knee joint HI2B is a good example of a part produced with a simple but professional technique. Handicap International (HI), an NGO, produces it in cooperation with the Sirindhorn National Medical Rehabilitation Centre in Thailand. Made of PVC, this joint can be produced for less than 200 baht(20) (approximately US$5.50) and requires less than a day for a technician to be trained to produce it, but it is of high enough quality to last at least a year.
Participants in a 1995 international conference in Phnom Penh on prosthetic technology observed that the most common failures in lower-limb prosthesis components are the following:
- Foot separation of the keel from the foot body; cracks, splits, and tears in the foam/latex; failure of the foot-ankle attachment.
- Knee extension stop wear/failure; bushing wear at the joint axis; cracks on and around the knee axis; wood degradation secondary to infestation, fungus, rot (this may also happen with glass-reinforced thermoplastic); failure of socket-knee interface.
- Socket material fatigue and stress fracture.
The participants concluded that a desirable overall life span for the knee of a prosthesis was two to three years. For the foot, they concluded that one and a half to two years would be acceptable(21). To make the foot more durable than this would significantly increase its weight.
Prosthetic feet
Imported prosthetic feet have been found deficient in Asian and Pacific developing countries for three reasons. First is the exorbitant cost of importing prosthetic feet from developed countries. Second, many imported feet have not been suitable for use in local cultural environments. Third, the imported feet are often not durable, especially under the rugged physical conditions in rural areas.
Most people in rural areas need to walk barefoot, work in fields, squat, sit on the ground and engage in manual tasks. They need a durable foot, preferably one that can last for significantly longer than a year under such conditions. Prosthetic feet currently being produced do not satisfy this requirement. Getting a new foot fitted annually may be a major disruption in the lives of some users, and may simply be impossible for others.

The solid-ankle-cushion-heel (SACH) foot is commonly used in the region, but it is not suitable for barefoot walking. It is also covered in polyurethane foam, which does not stay intact in hot climates.
The Mahavir Viklang Sahayta Samiti, an NGO based in Jaipur, India, developed the Jaipur Foot as a possible substitute for the SACH Foot. The Jaipur Foot is made of latex and microcellular (sponge) rubber (see the Technical Specifications Supplement for details of its production.) It is cheaper than the SACH Foot and well suited for squatting, cross-legged sitting, barefoot walking and even climbing trees. It is, however, heavier than the SACH Foot and designed primarily for use in an aluminium prosthesis. Furthermore, since all the steps in its production are manual, quality may vary from foot to foot.
Countries currently using Jaipur Feet include India and Sri Lanka. Most countries produce SACH Feet using the technique employed in making the Jaipur Foot (although some do not vulcanize the Foot).
Most NGOs in Cambodia use a rubber SACH Foot designed by Handicap International (HI). HI identified a privately-owned factory in Phnom Penh, which makes bicycle-wheel inner tubes and other rubber items. This factory now produces this Foot in large numbers. Another factory, which specializes in making plastic boilers for drinking water, produces the keel out of polypropylene with an injection machine.
The materials for the Foot are locally available. Polypropylene is recycled from prostheses and natural rubber comes from the Cambodian province of Kompong Cham. HI provided the technical support to both factories by transferring the relevant knowledge and supplying moulds, presses and a few other machines. Both these factories are likely to continue to meet the needs of Cambodians without further technical support from HI.
The Cambodian-made Foot pieces are also exported to the Lao People's Democratic Republic, Thailand and Viet Nam. The same design of Foot is now produced in Africa. The Government of Viet Nam plans to start the production of this Foot in Viet Nam in association with HI.
B. Orthoses

In some developing countries of the ESCAP region, the number of people with conditions that result in a need for orthoses (such as post-polio paralysis) is diminishing. In others, the number of people requiring orthoses is comparable to the number requiring prostheses. In both types of countries, however, parts for prostheses are more commonly produced than those for orthoses. There are, however, indications that the production of orthoses is increasing.
Many parts for orthoses can be made in workshops, but only in relatively limited quantities. Producing the parts in large numbers could achieve economies of scale, ensure uniform quality of parts and enable rehabilitation centres to produce orthoses in a shorter time than is presently the case. In India, parts are produced by the Artificial Limb Manufacturing Company (ALIMCO), a government corporation. They are distributed all over the country, as well as exported to neighbouring countries.
C. Wheelchairs and tricycles
Wheelchair production in many developing countries of the ESCAP region would be more cost-effective if it could take advantage of economies of scale already existing in the bicycle industry. This can be achieved by using standard bicycle parts, such as bicycle wheels, tyres and spokes, in the production of wheelchairs. The cost and production time required to obtain parts this way is considerably less than the cost of producing them specifically for wheelchairs. Countries with a strong bicycle industry are thus better equipped to produce wheelchairs.
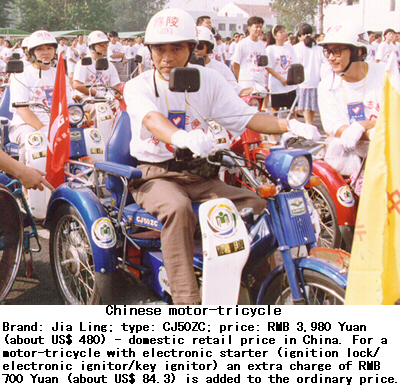
Tricycle manufacturers tend to buy most parts (usually bicycle parts) from outside rather than producing them in-house.
D. Devices for people with visual impairments
Assistive devices for people with visual impairments are not produced in many developing countries of the ESCAP region. Production of related parts, whether optical, electronic, electromagnetic or mechanical, is also limited, but some progress has been made. For example, speech synthesizers and optical character recognition packages in local languages have been produced in India and Thailand. The production of aspheric lenses, which can magnify images by more than five times without distortion, is being considered in India.
Braillers may require special spare parts to keep them in working order. Countries which make braillers are producing these parts. Their domestic production facilitates local maintenance and technical support for the devices.
E. Devices for people with hearing impairments
Assistive devices for people with hearing impairments make extensive use of electronic parts, which only a few developing countries of the ESCAP region can produce. Most developing countries in the region lack personnel with the necessary skills and expertise. Furthermore, batteries are a crucial part of many devices for people with hearing impairments. Most developing countries in the region import batteries although they are produced in the region. A similar situation exists concerning the production of the diagnostic equipment needed for the assessment of hearing loss.
Many parts, including transistors, simple integrated circuits, plastic cords, switches and connectors, are produced in China and India. However, receivers, microphones and special integrated circuits have to be imported even by those countries. Most of the listed parts have many applications and are not meant exclusively for use in equipment for people with hearing impairments.
20. Equivalent to approximately US$5.50 in September 1997.
21. Report of Syndicate D9.5, in report of ISPO (International Society for Prosthetics and Orthotics) Consensus Conference on Appropriate Prosthetic Technology for Developing Countries, held in Phnom Penh, 5-10 June 1995.
Box
Box 11: Dr. P.K. Sethi and the Jaipur Designs
Dr. P.K. Sethi is one of the inventors of the Jaipur prosthesis and its component, the Jaipur Foot. Dr. Sethi first thought of the idea for these devices in 1965, when he was prescribing solid-ankle-cushion-heel (SACH) feet to people with amputated lower limbs in Jaipur, India. He would ask users, in casual encounters outside the hospital setting, how satisfied they were with their new feet and found that many of them had returned to using crutches instead.
The production team had not realized that the SACH Foot, intended to be worn with shoes for sitting in chairs, was not suitable for Indians who walked barefoot and sat on the floor. By 1970, with the help of his fellow device producers, Dr. Sethi had the new designs which have since become known as the Jaipur prosthesis and Jaipur Foot.
As well as their cultural appropriateness, these devices have two other features that led to their popularity. First, they can be made easily by local artisans with local materials, so that once the design is known, they can be produced anywhere, not just in hospitals or other centres with specialized equipment and expertise. Second, Dr. Sethi's team did not patent the designs, making them available free of charge and thus reducing the cost to users. As a result, the devices have proved useful not only in the ESCAP region, but also in Africa, and Latin America.
Box 12: Parts for Different Lower-Limb Orthoses
| Type of orthosis | Abbrev. | Compensates for | Parts used |
| Hip Knee Ankle Foot Orthosis | HKAFO | Weakness and deformities in the hips and legs | Pelvic band, hip joint with lock, tuber band, thigh band, knee-joint bar assembly, knee joint, knee cap, calf band, ankle bar assembly, ankle joint, stirrup, footwear. |
| Knee Ankle Foot Orthosis | KAFO | Weakness in the portion of leg above the knee, the knee itself, the ankle and the foot | Tuber band, knee joint with lock, calf band, knee-joint bar assembly, ankle bar assembly, ankle joint, stirrup, insole, modified shoes. |
| Ankle Foot Orthosis | AFO | Weakness or deformities in the ankle, foot and the portion of leg below the knee | Calf band, ankle bar assembly, ankle joint, stirrup, insole, modified shoes. |
| Foot Orthosis | None | Deformities in the foot | Insole, modified shoes. |
Go back to the Contents
ECONOMIC AND SOCIAL COMMISSION FOR ASIA AND THE PACIFIC
Production and distribution of assistive devices for people with disabilities: Part 1
- Chapter 4 -
Printed in Thailand
November 1997 1,000
United Nations Publication
Sales No. E.98.II.F.7
Copyright c United Nations 1997
ISBN: 92-1-119775-9
ST/ESCAP/1774