INNOVATION, RESEARCH AND
DEVELOPMENT
This publication has noted (see Chapter V) that assistive devices imported from developed countries are often unsuitable for people with disabilities living under the physical, social, cultural and economic conditions of Asian and Pacific developing countries. For this reason, local research and development (R&D) and other forms of innovation are of crucial importance for the indigenous production of appropriate devices. This is not to say that developed countries can make no contribution to the development of assistive devices in Asian and Pacific developing countries. On the contrary, it is very important for developing countries to keep up with new knowledge about science, technology, manufacturing and new materials being generated in developed countries, in order to produce local solutions to local problems.
Furthermore, the import of technologies from developed countries has often had the benefit of stimulating local research. Typically, developing countries first adopt an assistive device by copying the design from developed countries (often modifying it just enough to avoid patent restrictions, so that the device can be produced at low cost). Over time, further local-level modifications are made, adapting the device to fit local conditions. This pattern has been observed with regard to the knee joints of AK prostheses, among other devices and components.
Laboratory-based R&D programmes involve considerable investment of funds for equipment, materials, components, energy and specialized expertise. Facilities for testing, making prototypes and field trials are also essential. Expensive laboratory R&D is not, however, the only kind of useful research in the field. Local innovation in the informal sector, often neglected by policy-makers, is central to the development of new devices and new methods of using them.
In addition, there is a middle level of research which, although conducted in an organized way under an official innovation budget, still does not require the equipment of a full scientific laboratory. Rural technologists and participants in CBR programmes are examples of those who may perform this kind of research. This is distinct from the more spontaneous adaptation to immediate needs that characterizes local innovation.
R&D efforts in the region, whether inside or outside the laboratory, often face the following difficulties:
- (a) Poor coordination;
- (b) Weak links with users;
- (c) Incorrect identification of needs;
- (d) Lack of appropriate inputs from specialized personnel;
- (e) Lack of funds.
In South Asia and South-East Asia, the growing trend is for countries to undertake their own R&D and to share the information within the subregions. Such trends should be encouraged in other subregions as well as among subregions.
A. Informal innovation
Since rehabilitation centres are rare in villages and remote areas of Asian and Pacific developing countries, people with disabilities in those areas, or their helpers, families or neighbours, have to develop appropriate assistive devices themselves.
The devices they produce are usually simple, small and effective. There are many examples of such informal innovation, especially in the field of mobility devices and devices for daily living. An example is the making and use, usually in a centre or workshop, of four-wheeled low-height trolleys for tetraplegic people to move about.
Those involved in introducing assistive devices invented in places away from the areas in which they are provided should remember to encourage local innovation as well. While there is a useful role for formal knowledge from outside a community, local people may easily produce an ingenious device that can be adapted for use in other places. Imported technology should be seen as a means of allowing innovation to focus on genuinely new devices. There is no need to reinvent the wheel or the wheelchair.
The main disadvantage of informal innovation is that, so far, there is lack of a mechanism for its propagation. This means that the innovation might not become as widely used as it could be. Replication could be easier in a small geographical area.
B. Participation of people with disabilities
No assistive device should be developed in the absence of consultation with and the participation of people with disabilities, who are the ultimate judges of whether a device is acceptable. Using sophisticated technology to design devices without user involvement may lead to the production of sophisticated devices with no relevance to users' lives and needs.
Knowledgeable people with disabilities who might potentially use the device in question must be consulted from the beginning of the design process. Users should be included directly as members of the decision-making team during the identification of needs, formulation and monitoring of projects, and assessment and evaluation of devices for use. Every device needs to be field-tested among a larger cross-section of potential users before it is produced and marketed.
Users will largely spell out their requirements qualitatively. For example, they may say that a hearing aid has a disturbance. The requirement of reducing the disturbance will have to be translated into quantitative terms by R&D scientists or engineers based on discussions with the users, in addition to the study of available equipment and technical literature. In the long term, it is desirable to train users in the higher-level skills for R&D, science and engineering.
C. Government subsidies and global trade regimes
The role of Government in promoting and supporting R&D is clearly established. This should continue for many more years in the region, especially in developing countries. Governments may have to provide subsidies directly or indirectly to industry and small- or medium-sized entreprises to support their production of assistive devices.
However, the global trade environment after the formation of the World Trade Organization (WTO) may impose some restrictions on the process of providing subsidies for the research, design, development and production of assistive devices. The Agreement on Subsidies and Countervailing Measures in the Uruguay Round, 1994, stipulates that subsidy to R&D will be non-actionable only if the following conditions laid down in the Agreement are met:
- Subsidy is non-specific i.e., not restricted to only a few enterprises, which might include public-sector industries;
- Financial support for research, in the case of specific subsidies, is restricted to some percentage of the total project cost.
As only a few industries are likely to engage in the research and production of assistive devices, Government support of those industries could be interpreted as actionable subsidy. If the norms mentioned in the Agreement are not satisfied, any member country of the WTO can raise objections to such a subsidy. This may affect government programmes to support people with disabilities. If the research is of a fundamental nature, it is outside the purview of the Agreement. Developing countries, including India, Indonesia, the Philippines and Sri Lanka, will not be affected for eight years (from January 1995); this is the transition period given to all member developing countries.
D. Patents and intellectual property
The case of the Jaipur prostheses, whose inventors freely transferred the necessary knowledge for production to many countries without receiving royalties, is an exceptional one. A more recent exception is the ground mobility device developed by the National Institute of Design, Ahmedabad, India.
More commonly, assistive devices are patented and their designers receive royalties on their use. A common mistake is the temptation to reinvent technology that is already freely available on a non-profit basis.
Rgimes of intellectual property rights are currently becoming stronger and more widely enforced. It is unlikely that assistive devices will be excluded. This presents both advantages and disadvantages for users of assistive devices. The advantage is that patent protection could potentially encourage more innovation and new designs of assistive devices. The disadvantage is that paying royalties will increase the cost of devices.
There is a danger that such cost increases may become prohibitive for buyers (be they users, NGOs or Governments). Some ways of preventing this exist:
- Even under wider patent rgimes, nothing prevents the inventor of a device from declining some or all royalties on humanitarian grounds, as in the case of the Jaipur prostheses and Ahmedabad ground-mobility device.
- Some assistive-device technologies are owned by Governments; these Governments can and should make the technologies available to benefit poor users in their countries and in other countries without charging royalties.
- Governments should create guidelines to ensure that sellers of assistive devices do not raise the prices by including the price of a technology which is no longer patented or is not directly related to the device under consideration.
E. Examples of national initiatives
1. China: A national R&D centre
Most R&D in China is carried out by the China Rehabilitation Research Centre (CRRC) in Beijing, as well as various universities around the country. The Governments of China and Japan jointly funded the setting up of the CRRC in 1988, each contributing US$25 million.
The CRRC is, so far, the only one of its kind in a developing country of the ESCAP region. It is dedicated exclusively to rehabilitation research and provides a clear focus to R&D activities in China. It includes a hospital and modern research facilities.
CRRC researchers are currently attempting to develop an intelligent knee joint, with a microprocessor to control the knee movement during the swing phase, as well as wheelchairs capable of climbing stairs. Such wheelchairs may also be useful for rough terrain. Reportedly, however, there is often a lack of funding for the actual production of the devices designed.
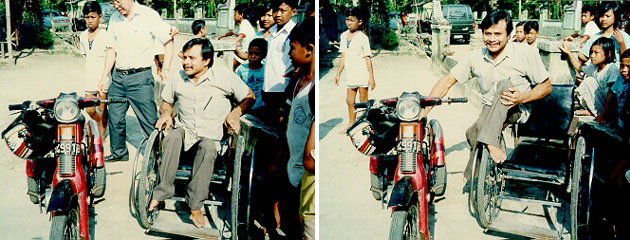
Various government factories produce the devices developed at the CRRC. One example is the petrol-fuelled tricycle, which may easily be observed on bicycle paths in China, driven by people with disabilities.
Some universities are also engaged in active research on assistive devices. The Shanghai Tongji University is developing hydraulic knee and hip joints, while the Shanghai Railway University is developing speech synthesizers in Chinese and braille keyboards. The Department of Precision Instruments and Mechanics at Qinghua University in Beijing has developed many devices currently under production, including titanium knee joints for AK prostheses and myoelectric hands.
2. India: A national research project
Indian efforts to promote R&D are broad-based and involve many agencies. One major Government of India initiative was the November 1988 launch of the Science and Technology Project in Mission Mode for the Welfare and Rehabilitation of the Handicapped, implemented primarily by the Ministry of Welfare.
The objective of the Project is to coordinate, fund and direct the development and utilization of suitable, cost- effective devices, as well as methods of education and skill development. The Project uses an interdisciplinary approach. In identifying areas of research, evaluating R&D proposals and monitoring their implementation progress, it involves:
- (a) At least seven concerned government ministries, departments and agencies;
- (b) Universities and research institutions;
- (c) Doctors;
- (d) Engineers;
- (e) People with disabilities;
- (f) Professionals in NGOs.
The government departments involved are the Ministry of Welfare, Department of Science and Technology, Department of Electronics, Planning Commission, Ministry of Health and Family Welfare, Ministry of Human Resource Development and Ministry of Labour.
Full R&D funding is provided to various agencies for project staff, equipment and services. A distinct feature of the Project is the support it provides to the private sector and NGOs, as well as public-sector institutions and programmes.
Areas of research are selected using the following methods:
- (a) Constant interaction with users and service providers;
- (b) Brainstorming sessions, workshops and seminars with experts;
- (c) Identification of laboratory-level technologies;
- (d) Evaluation of existing devices;
- (e) Study of the scientific and technical literature;
- (f) Assessment of available technical expertise;
- (g) Bestowing of national awards to the best inventions of assistive devices for their further development.
Interpointing braille writing frames, solar-powered chargers for hearing-aid batteries, feeding aids for children with cerebral palsy, and closed-circuit television with magnification facility for people with low vision are among the devices developed under the Project. They are now produced and provided in large numbers to users. Devices to prevent disabilities have also been developed, such as safety devices to minimize accidents in the use of farm machinery.
Different approaches have been used to transfer knowledge and technology to production and distribution centres and to users. The Government has subsidized production and distribution costs of devices developed in the Science and Technology Project to make them affordable to users.
For further details of this Project, see the India country paper in Part II: Madras Workshop Proceedings.
3. Thailand: Application of science and technology
The Department of Medicine at Chiang Mai University, Thailand, has developed a knee joint and a prosthesis for lower limbs in its workshop. These are now regularly used. The National Electronics and Computer Technology Centre, Ministry of Science and Technology, Bangkok, has started work on the development of an electric wheelchair.
Ratchasuda College, Bangkok, is working on the development of a Thai-language speech synthesizer. A project on developing a communication board for children with cerebral palsy and children with intellectual disabilities has also begun. A Thai-language optical character-recognition package has been successfully developed and is now available in the market. Most of the R&D work is being supported and funded by the Royal Thai Government.


Box
Box 17: Professor Jin Dewen

In the male-dominated field of assistive devices, it is rare for women to be involved in rehabilitation R&D ,especially in the design of state-of-the-art technology. Professor Jin Dewen is an exception. She is the Director of the Rehabilitation Centre in the department of Precision Instruments and Mechanics at Qinghua University in Beijing. Under her leadership, devices designed at the Centre include myoelectric forearm prostheses, energy-stroing prosthetic feet and super-stabilized knee joints. These knee joints help people with disabilities to engage in sports, walk on hilly ground and stand up from a sitting position.
Professor Jin has brought to her profession a high degree of sensitivity to user perspectives. It would benefit users of assistive devices if more such women became active in the research, design and development of assistive devices.
Go back to the Contents
ECONOMIC AND SOCIAL COMMISSION FOR ASIA AND THE PACIFIC
Production and distribution of assistive devices for people with disabilities: Part 1
- Chapter 9 -
Printed in Thailand
November 1997 1,000
United Nations Publication
Sales No. E.98.II.F.7
Copyright c United Nations 1997
ISBN: 92-1-119775-9
ST/ESCAP/1774