The 3rd Asia-Pacific CBR Congress
COMMUNITY BASED REHABILITATION AND ITS IMPACT ON QUALITY OF LIFE AND PSYCHOLOGICAL WELL-BEING AMONG PERSONS WITH DISABILITY
Background: Community Based Rehabilitation (CBR) focuses on enhancing the quality of life of person with disabilities and their families; meeting basic needs; protection of rights and ensuring inclusion and full participation in all aspects of community life. In absence of such interventions person with disabilities (PWDs) may develop psychological, economic and social problems, which have an adverse affect on life satisfaction, psychological well being and also on Quality of Life.
Objective: To assess the impact of livelihood component of CBR matrix on Psychological Well-Being and Quality of Life of PWDs.
Methods & Materials: The study comprises of 60 individuals with locomotor disability from two Blocks of Ranchi, Jharkhand, India. The impact of community based rehabilitation (CBR) on individual’s life was examined using the Socio-demographic data sheet, WHO Quality of Life (Saxena et al. 1998) and Psychological Well-Being (Dupuy, 1984). Ethical issues were followed while conducting study.
Results & Conclusion: CBR programs are also considered to be the most cost-effective approach to improve the wellbeing and increasing satisfaction level, in comparison with care in hospitals or rehabilitation centers. This model can also be used as a mental health promotion strategy for the person with disabilities. Study results will be discussed at the time of presentation.
Key Words: Community Based Rehabilitation (CBR), Mental Health, Quality of Life, Needs Satisfaction
1. M.Phil in Clinical Psychology (RCI No. A40059), CBR Consultant, Chotanagpur Sanskritik Sangh (CSS), Ranchi, Jharkhand, India.Email- nidhi_mehta@ymail.com Contact No. (+91) 9771343550
2. M.Ed (visual Impairment), Bachelor in Mental Retardation, Director, Health & Rehabilitation, CSS, Ranchi, India. Email- css.rncjh@gmail.com, Contact No. (+91) 9504900590
COMMUNITY BASED REHABILITATION AND ITS IMPACT ON QUALITY OF LIFE AND PSYCHOLOGICAL WELL-BEING AMONG PERSONS WITH DISABILITY
1. INTRODUCTION
The World Health Organisation (WHO) introduced the Community-Based Rehabilitation (CBR) strategy as part of its goal to accomplish health for all in 1978. The Alma-Ata Conference and Declaration of 1978 on Primary Health Care (PHC) created a new vision for providing promotive, preventive, curative and rehabilitative services for the main health problems in the community. But in last four decades the focus of CBR shifted from “Medical model” to “Human Rights model.”
The concept of CBR emerged in India during mid seventies. The development of CBR over the last 2 decades can be seen as a progression from a ‘service provider-beneficiary’ approach through a ‘service provider-client’ one, which is now moving towards a ‘client-owner’ emphasis. International policy statements now underscore the importance of rights and inclusion. Debates about ‘medical’ and ‘social’ models of disability gave way to a more universal understanding of the need for a comprehensive model. The main goals of CBR have become broader, and focus beyond the individual, to the community in which he/she lives. While these goals may be common across different contexts, the way they are translated into activities depend on the local situation, needs and resources. The recent approach on CBR states that it is a strategy within general community development for the rehabilitation, equalization of opportunities, and social inclusion of all people with disabilities. But all approaches and interventions do focus on “improvement in the Quality of Life”.
On 3rd October 2010 International Guideline for C.B.R. was declared with due emphasis on C.B.R. Matrix. Livelihood is one of the major components with Health, Education, Social and Empowerment. The Livelihood component focuses on Skill development, Self employment, Wage employment, Financial service and Social protection. This components aims that People with Disabilities gain a livelihood, have access to social protection measures and are able to earn enough income to lead dignified lives and contribute economically to their families and community. The role of CBR is to facilitate access for people with disabilities and their families to acquire skills, livelihood oppourtunities, enhance participation in community life and self-fulfilment. (CBR guideline, 2010).
Many Personal and environmental factors leads to impairment in body function and structures, restrictions in Activities and limitations on the participation which are directly related with Quality of life. The severity of disease causes variations in the daily needs of individuals and their families even in the same disability group. These disabilities cause limitations in activities and participation in adolescence and adulthood and affect the quality of life (QOL) and wellbeing in negative ways (Hetherington R, Dennis M, Barnes M, et al., 2002; Morris C, Kurinczuk JJ, Fitzpatrick R., 2005).
Well-being is a complex construct that encompasses multiple domains such as physical and mental health, happiness, and life satisfaction. Quality of life (QOL) is defined as individuals' perception of their position in life in context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns (World Health Organization Quality of Life Group.,1995). The unifying concept of quality of life enables service providers to reorganise resources around individuals rather than rearrange people in programme slots (Gardner JF, Nudler S and Chapman MS., 1997; Schalock R L, Brown I, Brown R, et al.,2002)
Individual QOL measures may be used for various purposes, including programme evaluation, research analysis, policy development, and meeting individualised needs (Rusch F R, H Hughes C and Hwang B., 1996).
Objective: To assess the impact of livelihood component of CBR matrix on Psychological Well-Being and Quality of Life of PWDs.
2. Review of Literature:-
Impact of livelihood has been studied by some researchers. Peter Coleridge states that unless disabled people have a voice, they will continue to be marginalised, misunderstood and excluded from poverty reduction strategies. CBR is identified as primarily a process of community, as well as individual, development, and is therefore an essential part of poverty reduction strategies (Peter Coleridge-2006).
Economic empowerment of PWDs is very crucial in raising their status. However, this cannot be achieved without the involvement and participation of all stakeholders: the government, members of the community, the labour market and PWDs themselves. CBR programmes need to increase sensitisation of the public on disability issues and rights of PWDs. Also, innovation and increased support for economic integration activities is necessary; as well as implementation of realistic and results-oriented plans in order to achieve successful empowerment of PWDs through CBR (Daniel Vershima Tsengu, Svein Brodtkorb, Torild Almnes-2006).
Among the evaluations featuring QOL, one (Powell A B, Mercer W S and Harte C., 2002) used Comprehensive-QOL Scale. Another (Cummins R A, McCabe M P, Romeo Y, et al., 1994) suggests that QOL was substantially lower among people with physical disabilities who received no rehabilitation services compared to those who did receive physical rehabilitation, Community Based Rehabilitation or labour market assistance. QOL scores tended to be highest, however, among those who received a combination of all three services.
CBR programmes are considered fundamental to improve the wellbeing of people with disabilities, and for fostering their participation in the community and society at large (Cornielje, 2009; Sharma, 2007). CBR programmes are also considered to be the most cost-effective approach to improve the wellbeing of people with disabilities, in comparison with care in hospitals or rehabilitation centres (Mitchell, 1999).
Alavi and Kuper (2010) identify a total of 51 studies evaluating the impact of rehabilitation of people with disabilities in Africa, Asia and Latin America (only two of these studies evaluating CBR programmes or services used a comparison group). Worldwide survey of researches and methods: literature is limited especially from an overall impact point of view. There are still no universally agreed criteria for the evaluation of CBR programmes (Finkenfugel et al., 2007)
3. METHODOLOGY:
3.1. Sample: 60 persons with loco-motor disability (severity ? 40%) who were having anyone of the five elements of livelihood component of CBR matrix under CBR programme by the NGO in Ranchi Jharkhand, India were selected through Purposive sampling technique.
| Elements | No. | Male | Female |
|---|---|---|---|
| Skill development | 12 | 06 | 06 |
| Self employment, | 12 | 06 | 06 |
| Wage employment, | 12 | 06 | 06 |
| Financial service | 12 | 06 | 06 |
| Social protection | 12 | 06 | 06 |
| N=60 | 30 | 30 |
Table 1: Frequency and % of participants Socio demographic Information (Categorical variables)
| S. No. | Domain | Responses | Frequency (%) N=60 |
|---|---|---|---|
| 1 | Gender | Male | 25 (41.7) |
| Female | 35 (58.3) | ||
| 2 | Religion | Hindu | 27(45.0) |
| Muslim | 15(25.0) | ||
| Christian | 09 (15.0) | ||
| Sarna | 09 (15.0) | ||
| 3 | Family Occupation | Agriculture activities | 32 (63.3) |
| Self employed | 20 (13.3) | ||
| Service Wage Employed | 12 (23.3) | ||
| 4 | Domicile | Rural | 28 (46.7) |
| Semi-Urban | 32 (53.3) | ||
| 4 | Socio-economic status | Lower | 35 (58.3) |
| Middle | 22 (36.7) | ||
| Higher | 03 (5.0) | ||
| 5 | Type of the family | Nuclear | 48 (80.0) |
| Joint | 12 (20.0) | ||
| 6 | Education | Primary | 32 (53.3) |
| Secondary | 20 (33.3) | ||
| Above | 08 (13.3) |
Table 1 shows that majority of the respondents were female 35 (58.3%) most of respondents from Hindu religion 27(45.0%). Majority of the persons with disability were engaging in agriculture 32 (63.3%). Most of the respondents were belongs to semi urban domicile 32 (53.3), 35 (58.3%) of respondents from lower socio economic status, 42(70.0%) most of the persons with disability belongs to nuclear family 48 (80%), most of the respondents education were up to primarily level 32 (53.3%).
| Variable | Mean (SD) N=60 |
|---|---|
| Age | 30.60 (5.97) |
| Income of Respondent- Per month | 4120.04 (1721.31) |
| Duration of assistance from CBR | 3.23 (1.75) |
3.2. Assessments
Socio demographic questionnaire
The information from each participant fulfilling the criteria was gathered through a detailed socio-demographic data sheet including age, gender, religion, caste, domicile, education, occupation, type of disability, and duration of assistance from CBR and NGO.
WHO Quality of Life (QOL)
The World Health Organization’s Quality of Life (QOL) is a measurement tool for the evaluation of quality of life. The scale includes 26 items asking about physical, psychological, social-relational, and environmental aspects of quality of life. Respondents were asked on the scale to make a subjective evaluation of their own lives using a 5-point Likert-type scale from 1(strongly disagree) to 5 (strongly agree). (Maximum score=130). Focus was on change due to livelihood programme.
It is a self-administered generic questionnaire developed in Hindi and shorter version of the WHO-QOL-100 scale which was developed as a measure that would be applicable cross-culturally. It lays emphasis on subjective evaluation of the respondent’s health, living condition and functioning and quality of life on the dimensions of physical, psychological, level of independence, social relations, environmental and spirituality/ religion/ personal belief. Each of these domains is treated as a separate numeric variable and higher the score, higher the quality of life. The scale has good reliability, comparable to that of WHO-QOL-100 scale (r?0.89). It also has good content and discriminate validity.Psychological General Well-Being
Psychological General Wellbeing Schedule (PGWS) (Dupuy,1984) measures a person’s subjective well-being. It is a self-reported questionnaire and it has 22 items which have six areas. Each item has 6 point (0-5) scales. Score for each affective group = SUM (points assigned for each question in group) where: the number in square brackets represent the points assigned for selected answer. Higher score indicate good psychological general well being in the each domain (Maximum score: 110)
3.3. Procedure
To conduct this study permission was taken from NGO named Chotanagpur Sanskritik Sangh based in Ranchi, Jharkhand, India. It is implementing CBR programme with the support of CBM. Researcher followed inclusion and exclusion criteria while selecting samples. Persons with loco-motor disability were deemed selected for the study only when they provided their written informed consent to the researcher. Information was collected in direct face-to-face interviews. Further WHO Quality of Life (Saxena et al. 1998) and Psychological Well-Being (Dupuy, 1984) was administered. Ethical issues were followed while conducting study.
3.4. Data analysis
The data obtained were analyzed with Statistical Package for Social Sciences-version 16.0 for Windows® (SPSS Inc., Chicago, IL, USA). The PGWB and WHO-QOL score was used for analysis.
3.5 Limitation of the Study:-
The sample size was also limited. Efforts were made to extract the impact of the livelihood component instead of general impact of CBR by explaining the respondent , but it was not a ‘controlled’ group.
4. Results
Table 1: Mean and Standard Deviation scores of QOL
| Variable | Skill development | Self employment | Wage employment | Financial service | Social protection | Mean (SD) N=60 |
|---|---|---|---|---|---|---|
| Physical QOL | 19.35 | 19.41 | 22.14 | 19.56 | 16.34 | 19.36 (4.34) |
| Psychological QOL | 16.35 | 17.20 | 16.90 | 16.45 | 15.60 | 16.50 (4.01) |
| Social QOL | 10.92 | 11.44 | 09.82 | 10.15 | 10.22 | 10.51 (2.94) |
| Environmental QOL | 17.32 | 17.14 | 16.54 | 16.35 | 16.15 | 16.70 (4.06) |
| Total score of QOL | 63.94 | 65.19 | 65.4 | 62.51 | 58.31 | 63.08 (8.81) |
| % of Score | 49.18 | 50.15 | 50.31 | 48.08 | 44.85 | 49.18 |
Table 1, shows the mean and SD score of Physical QOL was 19.36 (SD 4.34), psychological QOL was 16.50 (4.01), social QOL was 10.52 (2.94), environmental QOL was 17.70 (4.06), Overall Quality of Life (QOL) mean score was 63.08 (8.81). The mean score was 48.46%. It is considered as ‘good’ score; i.e. most of the PWD acknowledged improvement in quality of life due to interventions related to livelihood promotion.
The table reflects that the total score on QOL is highest by the people in Wage employment, followed by self employment. While it is lowest by the PWD in the element of Social protection. Persons in wage employment scored highest on Score on the QOL was on Physical wellbeing element was highest by while lowest in Social Well being. Persons in wage employment scored highest on Physical QOL while Persons in self employment scored highest on Psychological QOL and Social QOL. Persons under training scored highest in Environmental QOL.
Table 2: Mean and Standard Deviation scores of QOL
| Variable | Skill development | Self employment | Wage employment | Financial service | Social protection | Mean (SD) N=60 |
|---|---|---|---|---|---|---|
| Anxiety (lesser) | 16.84 | 16.94 | 16.96 | 16.85 | 16.81 | 16.88 (2.35) |
| Antidepressive mood | 11.44 | 11.43 | 11.41 | 11.42 | 11.55 | 11.45 (1.91) |
| Positive wellbeing | 15.36 | 15.41 | 15.37 | 15.32 | 15.19 | 15.33 (2.74) |
| Self control | 10.46 | 10.44 | 10.44 | 10.45 | 10.46 | 10.45 (1.62) |
| General health | 12.54 | 12.54 | 12.54 | 12.51 | 12.52 | 12.53 (1.83) |
| Vitality | 14.45 | 14.36 | 14.21 | 14.23 | 13.90 | 14.23 (2.06) |
| Total score of PGWB | 81.09 | 81.12 | 80.93 | 80.78 | 80.43 | 80.88 (7.49) |
| % of score | 73.72 | 73.75 | 73.57 | 73.44 | 73.12 | 53.52 |
Table 2, shows that mean and SD of anxiety domain was 16.88 (2.35), anti depressive mood was 11.45 (1.91), positive wellbeing 15.33 was (2.24), self control was 10.45 (1.62), general health was 12.53 (1.83), vitality was 14.23 (2.06), Overall psychological general wellbeing mean score was 80.88 (7.49). The highest score in the PGWB by PWD in self employment followed by PWD in Wage employment
5. DISCUSSION
The livelihood component, like every other component of CBR matrix, has very strong linkages with other components. Though all are important different components are ‘most important’ in specific age span and context. The QOL and PGWB tool indicates the subjective response of the PWDs and may be used as a tool for prioritizing the needs and interventions of CBR.
The current study found that the livelihood components of CBR matrix directly affect the QOL and Psychological well being of the persons with disability. Highest score in Physical QOL by PWD in wage employment reflects that physical well being may be improved by wage employment. While PWD under social protection, consider their physical well being not up to the mark, may be due to dependency on the Govt. Program.
PWD in Self employment have better social networking, social support, while those who are in wage employment still have poor social support. This indicates the possible discrimination and challenges for the PWDs who are in wage employment.
PWDs in the section of financial service were found least stable and anxious. The PWDs under training rated the environmental QOL better than other. This may be due the the structured setup of the training centres.
Present study findings reveals that persons with disability have adequate psychological wellbeing. The livelihood component of CBR contributes significantly in maintaining anxiety, checking depression and promoting Positive wellbeing, Self control, General health and Vitality.
It was also reflected that PWD in self employment are comparatively better in the psychological well being scale. The same findings was seen in Burns et al., (2007) as there was evidence that good work appears to help to improve mental health and wellbeing, the employment rate for people with mental health problems. Individual Placement and Support (IPS) is recognised in the literature as an effective rehabilitation programme for severe mental health problems (Burns et al., 2007)
Depression, lack of concentration, feelings of fatigue, loss of interest in daily activities, social isolation, and a sense of worthlessness were common feature of people living with disabilities (Healthy People, Disability and secondary conditions. 2002)
Many studies have reported that persons with disability having good quality of life due to acceptance of society about their existing problem is very helpful in having a normal life for the Persons with disability (Diener eat al., 1999).
A study conducted by Centres for Disease Control and Prevention (1989) found that if the disabled are motivated to appraise their health situation positively the adverse impact of disability could be reduced.
Persons with disabilities who are out of work, who cannot work, or whose resources from occupational activities are limited to maintain their livelihood have also limited access to financial services which inversely affects their QOL and PGWB.
Lesser score by the PWD in the Social protection reflects that the existing social protection schemes are not adequate to meet the livelihood needs of the PWDs.
5. CONCLUSION:
The Social and Empowerment components of CBR matrix are important for the improved Quality of Life of PWD but the contribution of ‘livelihood component’ is also significant. Wage employment contributes most in improving over all quality of life. However Self Employment contributes significantly in improving psychological well being along with improving QOL.
Under CBR programme livelihood components may be given specific priority. Skill training is a process while linkage with social protection schemes is a last option. Wage employment and Self- Employment must be given priority as per the individual needs and environment.
Quality of life and Psychological well being are directly correlated. It was also found that PWDs having more than one type of services score more. Therefore livelihood components of CBR programme must focus on Socio-psychological factors along with quality skill training and financial services.
Such study may be conducted with larger sample and scope.
References
- A hand book for parents of children with disabilities (2002).Planning Commission, Government of India, New Delhi
- Alavi Y. and Kuper H. (Eds.) (2010), Evaluating the Impact of Rehabilitation in the Lives of People with Disabilities and their Families in Low and Middle Income Countries A Review of Tools, London School of Hygiene & Tropical Medicine - UK, CBM – Germany.
- Cornielje H. (2009). The Role and Position of Disabled People’s Organisations in Community Based Rehabilitation: Balancing between Dividing Lines, Asia Pacific Disability Rehabilitation Journal, 20(1), 3-14.
- Cummins R A, McCabe M P, Romeo Y, Gullone E. The comprehensive quality of life scale: Instrument development and psychometric evaluation on tertiary staff and students. Educational and Psychological Measurement, 1994; 54:372-382.
- Diener E., Suh E.M., Lucas R.E. and Smith H.L, (1999) Subjective well-being: Three decades of progress. Psychological Bulletin, 125, 276–302.
- ESCAP. Understanding Community-Based Rehabilitation. Retrieved 18th March 2003, 1997, from http://www.unescap.org/decade/cbr.htm
- Felce D. Defining and applying the concept of quality of life. Journal of Intellectual Disability Research, 1997;41(2): 126-135.
- Finkenflügel, H., Cornielje, H. and Velema, J., (2008), The Use of Classification Models in the Evaluation of CBR Programmes, Disability and Rehabilitation, 30(5), 348-354
- Gardner JF, Nudler S, Chapman MS. Personal outcomes at measures of quality. Mental Retardation, 1997; 35:295-305.
- Govt insensitive to disabled children’s needs. Jalandhar, Jan 19. Available from: URL: http://www.tribuneindia.com/2012/20120120/jaltrib.htm
- Hetherington R, Dennis M, Barnes M, et al. Functional outcome in young adults with spina bifida and hydrocephalus. Childs Nerv Syst. 2006;22(2):117–24. [PubMed]
- ILO, UNESCO & WHO. Joint position paper on community-based rehabilitation with and for people with disabilities. Geneva. 2004.
- Mitchell R. (1999). The research base of community-based rehabilitation, Disability & Rehabilitation, 21 (10 & 11), 459 – 468
- Mitchell R. Community-based rehabilitation: the genaralized model. Disability and Rehabilitation, 1999; 21(10-11): 522-528.
- Morris C, Kurinczuk JJ, Fitzpatrick R. Child or family assessed measures of activity performance and participation for children with cerebral palsy:a structured review. Child Care Health Dev. 2005;31(4):397–407. [PubMed]
- Njini L, Goerdt A, Hanekom J, Lagerkvist B. Evaluation of Rehabilitation Services in Zimbabwe. Report from a mission jointly commissioned by the Ministry of Health, Zimbabwe and SIDA. Published by Ministry of Health; VA?llingby: Swedish Handicap Institute. 1991.
- Olivera R. Knowledge and attitude of Mothers with Disabled Children towards Community based Rehabilitation. RGUHS Journal of Nursing Sciences. May 2011.1 (1):28.
- Powell A B, Mercer W S, Harte C. (2002) Measuring the Impact of Rehabilitation Services on the Quality of Life of Disabled People in Cambodia.Disasters,;26(2): 175-191
- Rusch F R, H Hughes C, Hwang B. (1996)Attempts to conceptualize and measure quality of life. In R. L. Schalock (Ed.), Quality of life: Volume I. Conceptualization and measurement (pp. 51-61). Washington, DC: American Association on Mental Retardation.
- Schalock R L, Brown I, Brown R, Cummins R A, Felce D, Matikka L, et al. (2002)C.onceptualization, measurement, and application of quality of life for persons with intellectual disabilities: Report of an international panel of experts. Mental Retardation; 40(6):457-470.
- Sen A K. (1999) Development as Freedom (Oxford: Oxford University Press).
- Sharma, S., (2007), Community participation in community-based rehabilitation programmes, Asia Pacific Disability Rehabilitation Journal, 18(2), 146-157.
- Singh R. (2011).Social Stigmas Associated with Physically Disabled People. Youth Ki Awaaz.
- Vanneste G. (2001, January-February 2001). Editorial: Community Based Rehabilitation: What is it? Retrieved No. 6, fromhttp://www.disabilityworld.org/01-02_01/news/cbreditorial.htm
- WHO, ILO, UNESCO and IDDC (2010), Community-based Rehabilitation: CBR Guidelines, Towards Community-based Inclusive Development, Geneva.
- World Health Organization Quality of Life Group. The World Health Organization Quality of Life Assessment (WHOQOL): Position paper from the World Health Organization. Social Science Medicine, 1995;41(10): 1403-1409.
- World Health Organization. Declaration of Alma-Ata: World Health Organization. 1978.
- World Health Organization. Community Based Rehabilitation: Report of a WHO interregional consultation. Colombo, Sri Lanka, 28 June- 3 July. 1982. WHO (RHB/IR/82.1).
Slide 1 (Slide 1 text)
(Slide 1 text)
Slide 2 (Slide 2 text)
(Slide 2 text)
Slide 3 (Slide 3 text)
(Slide 3 text)
Slide 4 (Slide 4 text)
(Slide 4 text)
Slide 5 (Slide 5 text)
(Slide 5 text)
Slide 6 (Slide 6 text)
(Slide 6 text)
Slide 7 (Slide 7 text)
(Slide 7 text)
Slide 8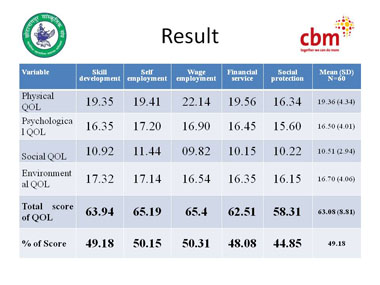 (Slide 8 text)
(Slide 8 text)
Slide 9 (Slide 9 text)
(Slide 9 text)
Slide 10 (Slide 10 text)
(Slide 10 text)
Slide 11 (Slide 11 text)
(Slide 11 text)
Slide 12 (Slide 12 text)
(Slide 12 text)
Slide 13 (Slide 13 text)
(Slide 13 text)
Slide 14 (Slide 14 text)
(Slide 14 text)
Slide 15 (Slide 15 text)
(Slide 15 text)
Slide 16 (Slide 16 text)
(Slide 16 text)
Slide 17 (Slide 17 text)
(Slide 17 text)
Slide 18 (Slide 18 text)
(Slide 18 text)
Slide 19 (Slide 19 text)
(Slide 19 text)
Slide 20 (Slide 20 text)
(Slide 20 text)
Slide 21 (Slide 21 text)
(Slide 21 text)
Slide 22 (Slide 22 text)
(Slide 22 text)
Slide 23 (Slide 23 text)
(Slide 23 text)