Web Posted on: August 24, 1998
The KommAS Communication Aid for Elderly People with Aphasia
Christian Bühler, Dirk Clemens, Helmut Heck, Rainer Wallbruch
Forschungsinstitut Technologie-Behindertenhilfe (FTB)
of Evangelische Stiftung Volmarstein,
Grundschötteler Straße 40,
D-58300 Wetter/Ruhr, Germany.
tel: + 49 (0) 2335 96810, fax: +49 (0) 2335 968119, email: sekr@ftb-volmarstein.de
1. Summary
The aim of the project 'KommAS' is to develop a computer-based communication aid for older people with severe aphasia that provides means for communication already in the beginning of the therapy. The system under development has to be adjusted to the special needs and interests of this person group with the help of integrated special tools like mnemonic aids or exercises. So even older people with aphasia will be enabled to take part in the community again.
| Top |
2. Introduction
Predominantly older people fall ill with aphasia. They mainly suffer from cerebrovascular accidents or cerebral atrophies which are the most frequent causes of aphasia. Other causes are head injuries, cerebral tumours and encephalitides, which attack areas in the speech centre of the brain. Resulting from neurological damage, expression and comprehension of spoken and written language are affected in different ways. All modalities - speaking, understanding, reading and writing - are affected partly in different extensions.
Especially for older people it often leads to exclusion and social isolation that the verbal communication is either more difficult or totally inhibited.
There are problems with the use of AAC devices in the group of people with aphasia which result from the loss of fundamental language structuring skills because in addition to the spoken language skills, text, and symbolic language skills may be impaired, too.
It is shown that the sooner speech therapy begins the better are the achieved improvements and the greater is a chance for recovery of social integration and gainful employment. Specific speech therapy usually can achieve a clear improvement even if a chronic aphasia is lasting for years [1].
The use of a communication aid within an AAC intervention [2] could be part of an aphasia treatment. The various approaches in aphasia therapy come to different conclusions about the use of a communication aid. Recently there was a change from early traditional deficit reduction approaches in therapy to more 'functional' approaches where communication needs and the way of life of the aphasic people are more considered. Fox and Fried-Oken [3] give an overview about different approaches currently used in aphasia therapy.
| Top |
3. Aim of the KommAS project
In form of a portable prototype a computer based communication system for people with aphasia is being developed. The system also supports speech therapy. Therefore it integrates features for self-determined speech exercises. This exercises can be performed at home without the presence of a therapist. Additionally memory supporting functions facilitate managing of all day situations, e.g. shopping, dates. A model of the tasks and relationship of the system is shown in Figure 1.
General design goals for AAC, as Goodenough-Trepagnier [4] suggested, have to be considered in the development, i.e. learnability, consistency, immediate utility, spontaneity, minimum motor demand, minimum attention shifting, and goals that fit people.
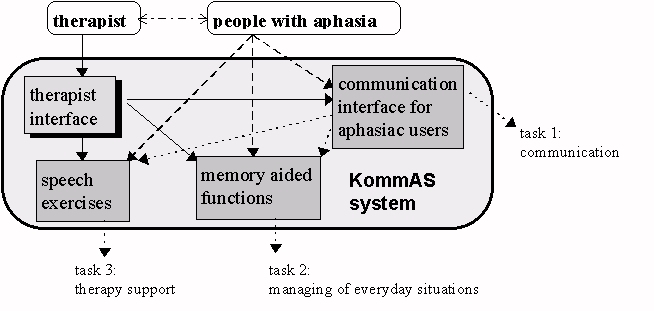
Figure 1: Model of tasks and relationship of the KommAS system
| Top |
4. Procedures
For an extensive analysis of user requirements various persons were interviewed: therapists, self-help groups and patients. This analysis based on open and structured interviews yielded the following results: there should be two kinds of user interfaces, one for the therapist and one for the person affected by aphasia. Wide configuration possibilities are needed because the treatment during therapy is symptom specific and is therefore aimed at the individual needs. This goes equally for both, the personal communication interfaces and possibly personal exercises. Another topic which has to be considered is the configuration time: therapists wish to create new user menus very quickly. They will apply a large library of symbols, pictures, videos and sounds. For a better acceptance and easy recognition therapists may want to build in photographs of the known environment. The access of this visual material is realised through keywords. Each tool should work in the usual way: with mouse drag & drop, hot keys and other well known tricks. It may be appropriate for the therapists to block some of the built-in functions for the aphasic people to prevent overexertion. This applies to all tasks which the client with aphasia may use, the communication interface, the speech exercises, and the memory aided functions. In contrast to this the people with aphasia want to configure and to optimise their interfaces on their own. Because there may be motoric problems, e.g. some of the users have only the ability to control one single button or sensor, the handling, configuration and optimisation of the user interface will work with scanning as well as with pointing devices.
Required techniques for an easy communication with an extensive and flexible vocabulary are, for example, the use of different levels [2], the use of abbreviation expansion and the use of predictive techniques [5].
A field test is planned with an evaluation of the prototype systems after the development. The systems will be proven with regard to their applicability. Therapists and persons affected by aphasia in various institutions will be employed in testing the prototype.
| Top |
5. Implementation
The implementation is done in C++. The software runs under Microsoft Windows 3.1 and Windows 95. We have implemented the scanning mode for all standard windows elements like scroll bars, radio buttons and push buttons. Menus will be displayed as dialogue boxes. Scanning mode means, that after a time interval the computer selects the next entry. The user must press (with hand, foot, head, neck, ...) the button if he will modify or activate the entry. The software supports also a scanning mode with two buttons. With the first button the user selects the next element, with the second button he will modify or activate the selected object. Mostly everything may be controlled by mouse, keyboard or with only one single button. Because of this, people with disabilities may configure their own human-machine-interfaces.
The human-machine-interface consists of many different views. Each view may contain different pictures, graphics and OLE objects, which may be placed anywhere in the view. Other views may also be visible in the view. Some of these objects may be grouped together and would be handled as one object. Each object may be linked to a sound or a video sequence.
With mouse control the user can click the objects directly. In scanning mode all objects will be selected one by one. If an object has been activated and there is a sound or/and video linked to the object, it/they is/are played. If the selected object is a group of objects, the scanning mode continues within this group. If the selected object is another view, this new view will be displayed instead of the current one.
The views can be linked in different ways together, perhaps like trees with the behaviour of menus and submenus, like link-lists, or like anything else. Some assistants will help the user to configure the views.
A library with many photos, pictures, videos and sounds will be integrated into this system. The library with the symbols, pictures and videos is implemented as a keyword related database. Every visual material takes one or more keywords. If a user searches for 'hand', he gets a sorted list with many 'hands' and must only select one of them. The library can be expanded by the user.
| Top |
6. Example of a program tool
An example of additional functions, one part of the program, a daytime planning help is shown in Figure 2.
The day time managing module was implemented in order to help the persons with aphasia by fixing and recognising of dates and of recognising sequences of events. The user can choose different functions like: showing dates or sequences of events, changing or editing dates, and showing tips, which means a further explanation to one date. This e.g. could be the address of the doctor or a description of the way to him.
On all day-time-planner pages the actual date and time is shown in the right corners. In the figure, the page to edit dates is shown. On the first row, pictures represent a category like doctors in this example. In the second row we have an icon for the family doctor, for the dentist, the radiologist and other subcategories.
Pictures at the left side show the kind of appointments which can be chosen by pressing the icon for the category and the icon for the subcategory.
Pressing the number buttons on the top chooses the day, pressing a number button at the bottom chooses the time of an appointment. Day or time can also be changed by pressing the 'up'- and 'down'-buttons.Chosen kind, date, and time of a date are represented in the middle of the window.
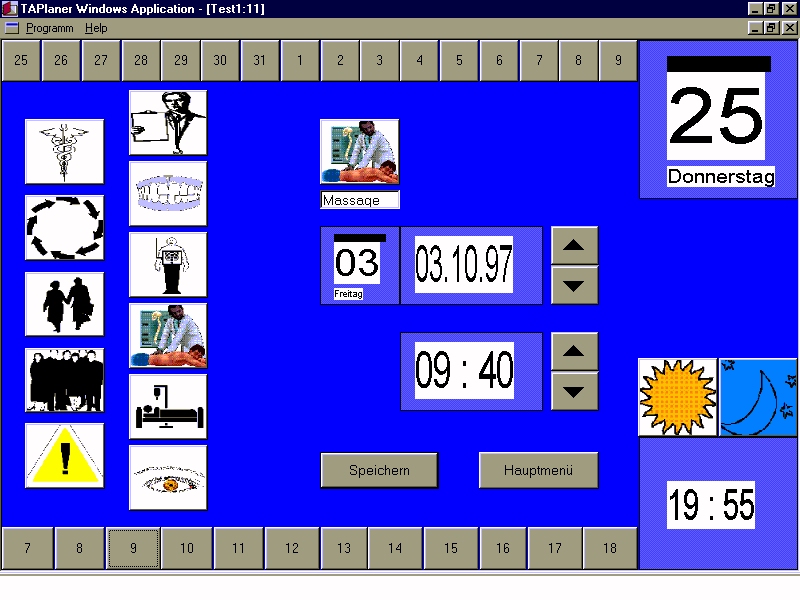
Figure 2: Example of an additional mnemonic tool of the KommAS system: a day time manager
| Top |
7. Acknowledgement
The KommAS project is supported by the German Federal Minister for Family, Elderly, Women, and Youth.
| Top |
Literature:
[1] H.-A. Linck, M. Fröscher, Medizinische Grundlagen der Aphasien. In: Bundesarbeitsgemeinschaft Hilfe für Behinderte e.V. (Hrsg.), Kommunikation zwischen Partnern. Schriftenreihe der Bundesarbeitsgemeinschaft Hilfe für Behinderte, Band 240. Düsseldorf 1986, 8-20.
[2] Bühler, C.; Heck, H.; Wallbruch, R.: Effective communication with BASCO: Smart text version in German. In: Conference Book and Proc.s of the Sixth Biennial Conf. of ISAAC; pp. 484-487; MECC, Maastricht, the Netherlands, October 9-13, 1994.
[3] Lynn E. Fox and Melanie Fried-Oken, AAC Aphasiology: Partnership for Future Research. AAC Augmentative and Alternative Communication 12 (Dec. 1996) 257-271.
[4] C. Goodenough-Trepagnier, Design Goals for Augmentative Communication. Assistive Technology 6.1 (1994) 3-9.
[5] C. R. Musslewhite and K. W. St.Louis, Communication Programming for Persons with severe Handicaps: vocal and augmentative strategies. Austin, Texas: Pro ed, 1988, pp. y279-285.
| Top | | TIDE 98 Papers |